

Fluorodeoxyglucose-positron emission tomography scan-positive recurrent papillary thyroid cancer and the prognosis and implications for surgical management
- PMID: 22985118
- PMCID: PMC3539949
- DOI: 10.1186/1477-7819-10-192
Fluorodeoxyglucose-positron emission tomography scan-positive recurrent papillary thyroid cancer and the prognosis and implications for surgical management
Abstract
Background: To compare outcomes for patients with recurrent or persistent papillary thyroid cancer (PTC) who had metastatic tumors that were fluorodeoxyglucose-positron emission tomography (FDG-PET) positive or negative, and to determine whether the FDG-PET scan findings changed the outcome of medical and surgical management.
Methods: From a prospective thyroid cancer database, we retrospectively identified patients with recurrent or persistent PTC and reviewed data on demographics, initial stage, location and extent of persistent or recurrent disease, clinical management, disease-free survival and outcome. We further identified subsets of patients who had an FDG-PET scan or an FDG-PET/CT scan and whole-body radioactive iodine scans and categorized them by whether they had one or more FDG-PET-avid (PET-positive) lesions or PET-negative lesions. The medical and surgical treatments and outcome of these patients were compared.
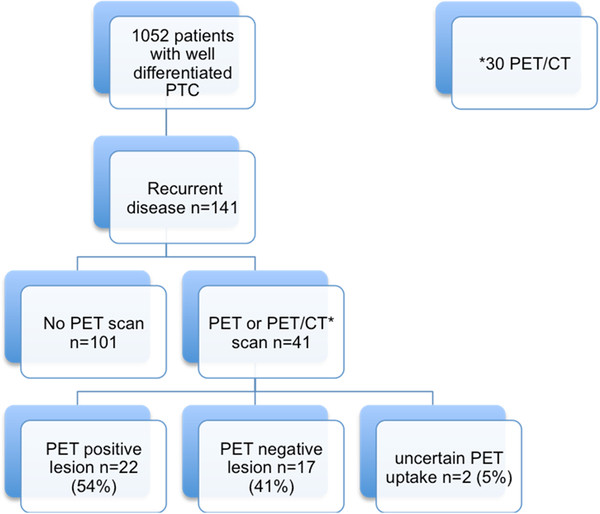
Results: Between 1984 and 2008, 41 of 141 patients who had recurrent or persistent PTC underwent FDG-PET (n = 11) or FDG-PET/CT scans (n = 30); 22 patients (54%) had one or more PET-positive lesion(s), 17 (41%) had PET-negative lesions, and two had indeterminate lesions. Most PET-positive lesions were located in the neck (55%). Patients who had a PET-positive lesion had a significantly higher TNM stage (P = 0.01), higher age (P = 0.03), and higher thyroglobulin (P = 0.024). Only patients who had PET-positive lesions died (5/22 vs. 0/17 for PET-negative lesions; P = 0.04). In two of the seven patients who underwent surgical resection of their PET-positive lesions, loco-regional control was obtained without evidence of residual disease.
Conclusion: Patients with recurrent or persistent PTC and FDG-PET-positive lesions have a worse prognosis. In some patients loco-regional control can be obtained without evidence of residual disease by reoperation if the lesion is localized in the neck or mediastinum.
Figures
Similar articles
-
Postoperative fluorine-18-fluorodeoxyglucose positron emission tomography/computed tomography: an important imaging modality in patients with aggressive histology of differentiated thyroid cancer.Thyroid. 2015 Apr;25(4):437-44. doi: 10.1089/thy.2014.0320. Epub 2015 Mar 16. Thyroid. 2015. PMID: 25633259
-
Prognostic implication of fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography in patients with recurrent papillary thyroid cancer.Head Neck. 2018 Jan;40(1):94-102. doi: 10.1002/hed.24967. Epub 2017 Nov 11. Head Neck. 2018. PMID: 29130586
-
Impact of FDG-PET computed tomography for surgery of recurrent or persistent differentiated thyroid carcinoma.Horm Metab Res. 2012 Nov;44(12):904-8. doi: 10.1055/s-0032-1316351. Epub 2012 Jul 12. Horm Metab Res. 2012. PMID: 22791600
-
Respective roles of thyroglobulin, radioiodine imaging, and positron emission tomography in the assessment of thyroid cancer.Semin Nucl Med. 2006 Jul;36(3):194-205. doi: 10.1053/j.semnuclmed.2006.03.002. Semin Nucl Med. 2006. PMID: 16762610 Review.
-
Value of Fluorodeoxyglucose PET/Computed Tomography Patient Management and Outcomes in Thyroid Cancer.PET Clin. 2015 Apr;10(2):265-78. doi: 10.1016/j.cpet.2014.12.009. Epub 2015 Jan 29. PET Clin. 2015. PMID: 25829091 Review.
Cited by
-
Prognostic role of FDG PET/CT in patients with differentiated thyroid cancer treated with 131-iodine empiric therapy.Medicine (Baltimore). 2017 Oct;96(42):e8344. doi: 10.1097/MD.0000000000008344. Medicine (Baltimore). 2017. PMID: 29049252 Free PMC article.
-
Treatment strategies for radioactive iodine-refractory differentiated thyroid cancer.Ther Adv Med Oncol. 2014 Nov;6(6):267-79. doi: 10.1177/1758834014548188. Ther Adv Med Oncol. 2014. PMID: 25364392 Free PMC article. Review.
-
Use of imaging tests after primary treatment of thyroid cancer in the United States: population based retrospective cohort study evaluating death and recurrence.BMJ. 2016 Jul 20;354:i3839. doi: 10.1136/bmj.i3839. BMJ. 2016. PMID: 27443325 Free PMC article.
-
[18F]-FDG Uptake as a Marker of Residual Anaplastic and Poorly Differentiated Thyroid Carcinoma following BRAF-Targeted Therapy.AJNR Am J Neuroradiol. 2025 Jun 3;46(6):1260-1267. doi: 10.3174/ajnr.A8588. AJNR Am J Neuroradiol. 2025. PMID: 39572200
References
-
- Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Sherman SI, Tuttle RM. American Thyroid Association Guidelines Taskforce. Management guidelines of patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2006;16:109–142. doi: 10.1089/thy.2006.16.109. - DOI - PubMed
-
- Rouxel A, Hejblum G, Bernier MO, Boelle PY, Menegaux F, Mansour G, Hoang C, Aurengo A, Leenhardt L. Prognostic factors associated with the survival of patients developing loco-regional recurrences of differentiated thyroid carcinomas. J Clin Endocrinol Metab. 2004;89:5362–5368. doi: 10.1210/jc.2003-032004. - DOI - PubMed
-
- Giammarile F, Hafdi Z, Bournaud C, Janier M, Houzard C, Desuzinges C, Itti R, Sassolas G, Borson-Chazot F. Is [18 F]-2-fluoro-2-deoxy-d-glucose (FDG) scintigraphy with non-dedicated positron emission tomography useful in the diagnostic management of suspected metastatic thyroid carcinoma in patients with no detectable radioiodine uptake? Eur J Endocrinol. 2003;149:293–300. doi: 10.1530/eje.0.1490293. - DOI - PubMed
