

Low-dose hydroxychloroquine is as effective as phlebotomy in treatment of patients with porphyria cutanea tarda
- PMID: 22985607
- PMCID: PMC3501544
- DOI: 10.1016/j.cgh.2012.08.038
Low-dose hydroxychloroquine is as effective as phlebotomy in treatment of patients with porphyria cutanea tarda
Abstract
Background & aims: Porphyria cutanea tarda (PCT) is an iron-related disorder caused by reduced activity of hepatic uroporphyrinogen decarboxylase; it can be treated by phlebotomy or low doses of hydroxychloroquine. We performed a prospective pilot study to compare the efficacy and safety of these therapies.
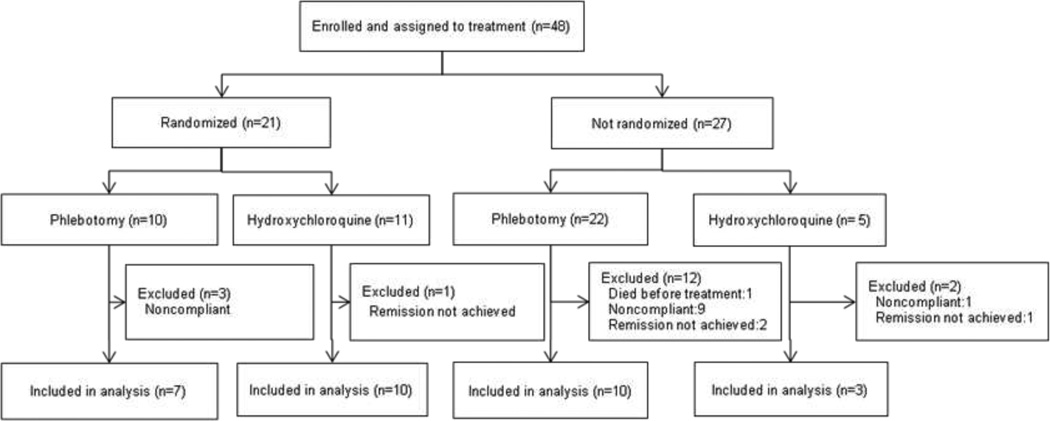
Methods: We analyzed data from 48 consecutive patients with well-documented PCT to characterize susceptibility factors; patients were treated with phlebotomy (450 mL, every 2 weeks until they had serum ferritin levels of 20 ng/mL) or low-dose hydroxychloroquine (100 mg orally, twice weekly, until at least 1 month after they had normal plasma levels of porphyrin). We compared the time required to achieve a normal plasma porphyrin concentration (remission, the primary outcome) for 17 patients treated with phlebotomy and 13 treated with hydroxychloroquine.
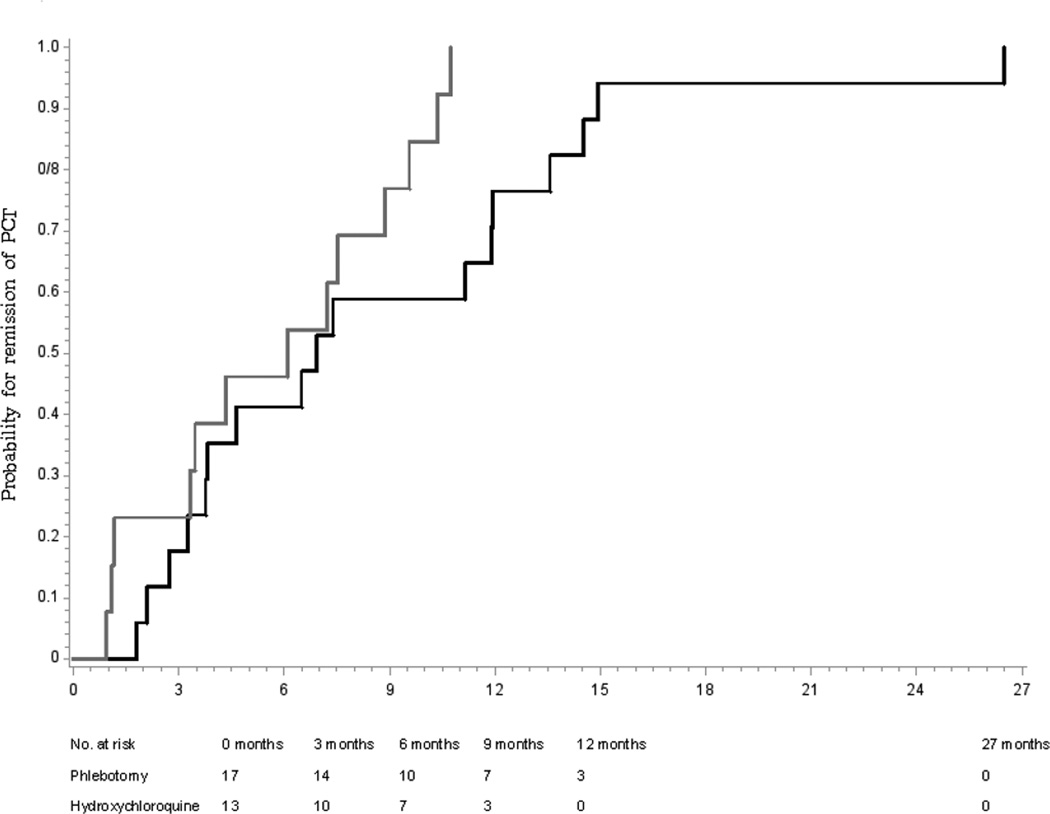
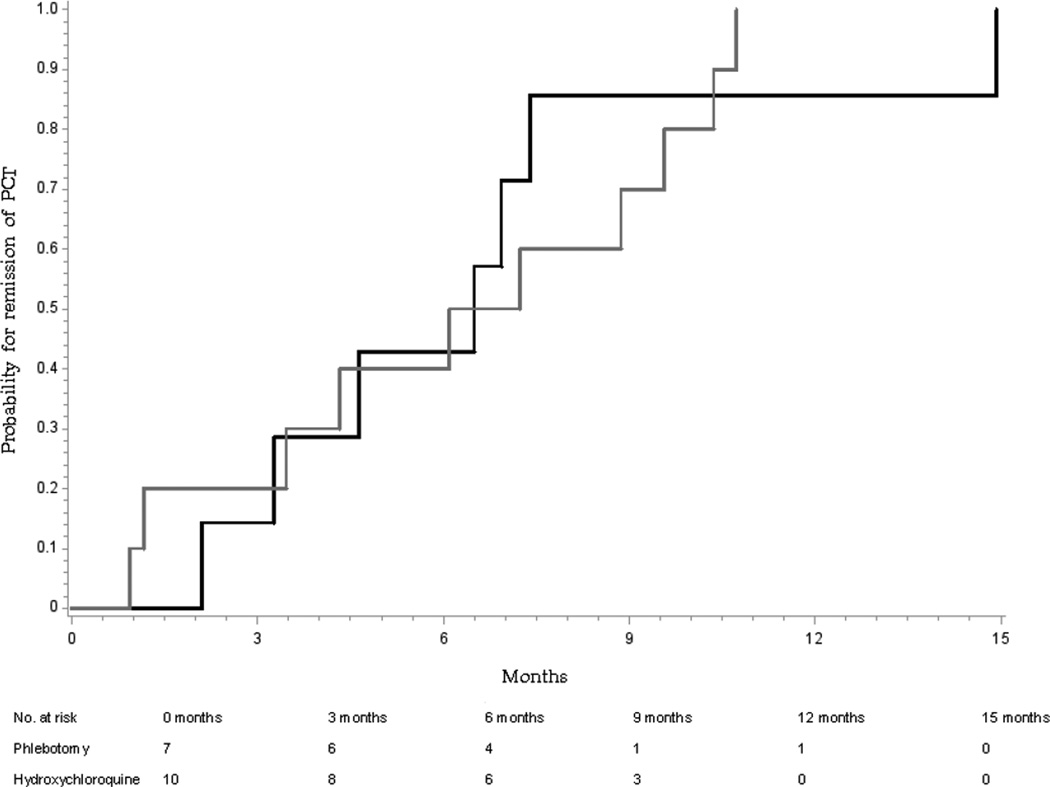
Results: The time to remission was a median 6.9 months for patients who received phlebotomy and 6.1 months for patients treated with hydroxychloroquine treatment (6.7 and 6.5 mo for randomized patients), a difference that was not significant (log-rank, P = .06 and P = .95, respectively). The sample size was insufficient to confirm noninferiority of hydroxychloroquine treatment (hazard ratio, 2.19; 95% confidence interval, 0.95-5.06) for all patients. Patients who received hydroxychloroquine had substantially better compliance. There were no significant side effects of either treatment.
Conclusions: Hydroxychloroquine, 100 mg twice weekly, is as effective and safe as phlebotomy in patients with PCT, although noninferiority was not established. Given these results, higher-dose regimens of hydroxychloroquine, which have more side effects, do not seem justified. Compliance was better and projected costs were lower for hydroxychloroquine than phlebotomy treatment. Long-term studies are needed to compare durability of response. ClinicalTrials.gov number, NCT01573754.
Copyright © 2012 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Porphyria cutanea tarda: treatment options revisited.Clin Gastroenterol Hepatol. 2012 Dec;10(12):1410-1. doi: 10.1016/j.cgh.2012.09.005. Epub 2012 Sep 13. Clin Gastroenterol Hepatol. 2012. PMID: 22982098 No abstract available.
References
-
- Elder GH. Porphyria cutanea tarda and related disorders (Chapter 88) In: Kadish KM, Smith K, Guilard R, editors. Porphyrin Handbook, Part II. Volume 14. San Diego: Academic Press; 2003. pp. 67–92.
-
- Lundvall O, Weinfeld A, Lundin P. Iron storage in porphyria cutanea tarda. Acta Med Scand. 1970;188:37–53. - PubMed
-
- Sampietro M, Fiorelli G, Fargion S. Iron overload in porphyria cutanea tarda. Haematologica. 1999;84:248–253. - PubMed
-
- Bygum A, Brandrup F, Christiansen L, Petersen NE. [Porphyria cutanea tarda] Ugeskr Laeger. 2000;162:2020–2024. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
