

Comprehensive smoking bans and acute myocardial infarction among Medicare enrollees in 387 US counties: 1999-2008
- PMID: 22986145
- PMCID: PMC3530376
- DOI: 10.1093/aje/kws267
Comprehensive smoking bans and acute myocardial infarction among Medicare enrollees in 387 US counties: 1999-2008
Abstract
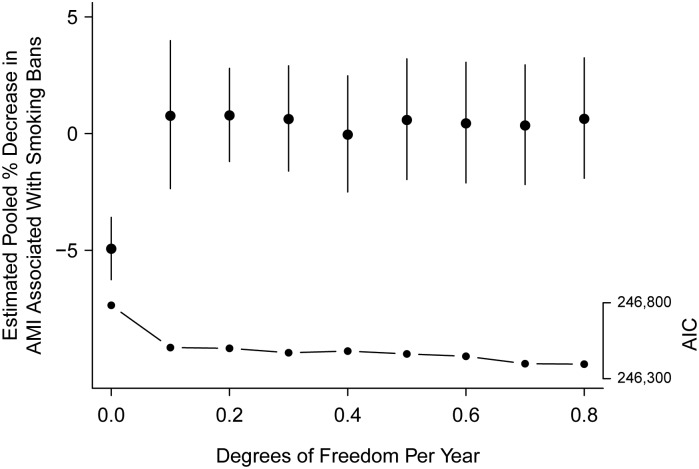
Restrictions on smoking in public places have become increasingly widespread in the United States, particularly since the year 2005. National-scale studies in Europe and local-scale studies in the United States have found decreases in hospital admissions for acute myocardial infarction (AMI) following smoking bans. The authors analyzed AMI admission rates for the years 1999-2008 in 387 US counties that enacted comprehensive smoking bans across 9 US states, using a study population of approximately 6 million Medicare enrollees aged 65 years or older. Effects of smoking bans on AMI admissions were estimated by using Poisson regression with linear and nonlinear adjustment for secular trend and random effects at the county level. Under the assumption of linearity in the secular trend of declining AMI, smoking bans were associated with a statistically significant ban-associated decrease in admissions for AMI in the 12 months following the ban. However, the estimated effect was attenuated to nearly zero when the assumption of linearity in the underlying trend was relaxed. This analysis demonstrates that estimation of potential health benefits associated with comprehensive smoking bans is challenged by the need to adjust for nonlinearity in secular trend.
Figures


References
-
- US Public Health Service. Smoking and Health: Report of the Advisory Committee to the Surgeon General of the Public Health Service. Washington, DC: Office of the Surgeon General, US Public Health Service; 1964. (DHEW publication no. (PHS) 1103)
-
- US Department of Health and Human Services. The Health Consequences of Involuntary Smoking: A Report of the Surgeon General. Rockville, MD: Office of Smoking and Health, Department of Health and Human Services; 1986.
-
- Law MR, Morris JK, Wald NJ. Environmental tobacco smoke exposure and ischaemic heart disease: an evaluation of the evidence. BMJ. 1997;315:973–980. doi:10.1136/bmj.315.7114.973. - DOI - PMC - PubMed
-
- Barnoya J, Glantz SA. Cardiovascular effects of secondhand smoke: nearly as large as smoking. Circulation. 2005;111:2684–2698. doi:10.1161/CIRCULATIONAHA.104.492215. - DOI - PubMed
-
- US Department of Health and Human Services. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General. Atlanta, GA: Office of Smoking and Health, US Department of Health and Human Services; 2006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
