

Lymph nodes and survival in pancreatic neuroendocrine tumors
- PMID: 22987171
- PMCID: PMC3448121
- DOI: 10.1001/archsurg.2012.1261
Lymph nodes and survival in pancreatic neuroendocrine tumors
Abstract
Hypothesis: Lymph node metastases decrease survival in patients with pancreatic neuroendocrine tumors (pNETs).
Design: Prospective database searches.
Setting: National Institutes of Health (NIH) and Stanford University Hospital (SUH).
Patients: A total of 326 patients underwent surgical exploration for pNETs at the NIH (n = 216) and SUH (n = 110).
Main outcome measures: Overall survival, disease-related survival, and time to development of liver metastases.
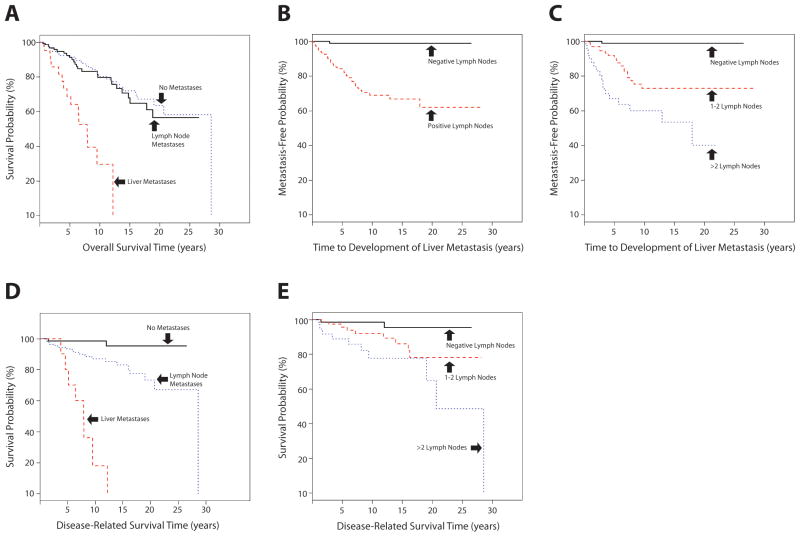
Results: Forty patients (12.3%) underwent enucleation and 305 (93.6%) underwent resection. Of the patients who underwent resection, 117 (35.9%) had partial pancreatectomy and 30 (9.2%) had a Whipple procedure. Forty-one patients also had liver resections, 21 had wedge resections, and 20 had lobectomies. Mean follow-up was 8.1 years (range, 0.3-28.6 years). The 10-year overall survival for patients with no metastases or lymph node metastases only was similar at 80%. As expected, patients with liver metastases had a significantly decreased 10-year survival of 30% (P < .001). The time to development of liver metastases was significantly reduced for patients with lymph node metastases alone compared with those with none (P < .001). For the NIH cohort with longer follow-up, disease-related survival was significantly different for those patients with no metastases, lymph node metastases alone, and liver metastases (P < .001). Extent of lymph node involvement in this subgroup showed that disease-related survival decreased as a function of the number of lymph nodes involved (P = .004).
Conclusions: As expected, liver metastases decrease survival of patients with pNETs. Patients with lymph node metastases alone have a shorter time to the development of liver metastases that is dependent on the number of lymph nodes involved. With sufficient long-term follow-up, lymph node metastases decrease disease-related survival. Careful evaluation of number and extent of lymph node involvement is warranted in all surgical procedures for pNETs.
Figures
Comment in
-
When pNETs bust out of their shells.Arch Surg. 2012 Sep;147(9):828. doi: 10.1001/archsurg.2012.1281. Arch Surg. 2012. PMID: 22987172 No abstract available.
References
-
- Vortmeyer AO, Huang S, Lubensky I, Zhuang Z. Non-islet origin of pancreatic islet cell tumors. J Clin Endocrinol Metab. 2004 Apr;89(4):1934–1938. - PubMed
-
- Rindi G, Wiedenmann B. Neuroendocrine neoplasms of the gut and pancreas: new insights. Nat Rev Endocrinol. 2011 Aug 2; - PubMed
-
- Jensen RT, Delle Fave G. Promising advances in the treatment of malignant pancreatic endocrine tumors. N Engl J Med. 2011 Feb 10;364(6):564–565. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
