

Improving delivery of EPSDT well-child care at acute visits in an academic pediatric practice
- PMID: 22987871
- PMCID: PMC9923557
- DOI: 10.1542/peds.2012-0355
Improving delivery of EPSDT well-child care at acute visits in an academic pediatric practice
Abstract
Background and objective: Many patients with Medicaid do not receive timely, comprehensive well-child care through the Early and Periodic Screening, Diagnosis, and Treatment (EPSDT) program. Missed opportunities for EPSDT well-child check-ups (WCCs) at acute visits contribute to this problem. The authors sought to reduce missed opportunities for WCCs at acute visits for patients overdue for those services.
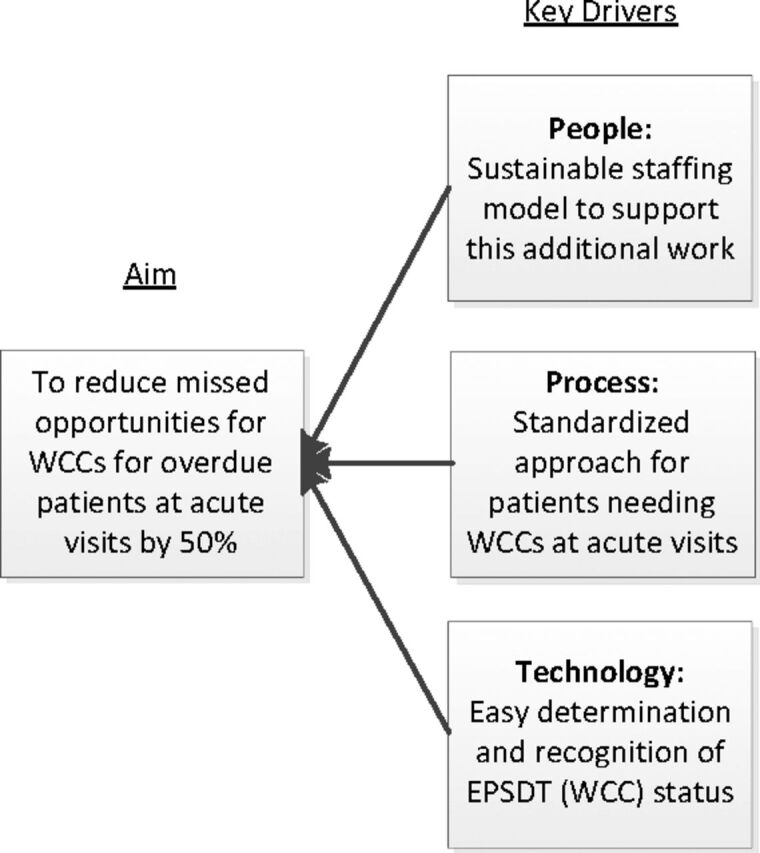
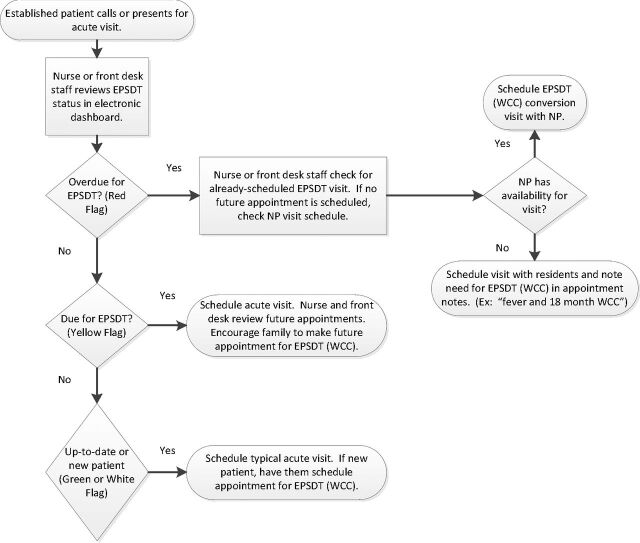
Methods: A quality improvement team developed key drivers and used a people-process-technology framework to devise 3 interventions: (1) an electronic indicator based on novel definitions of EPSDT status (up-to-date, due, overdue, no EPSDT), (2) a standardized scheduling process for acute visits based on EPSDT status, and (3) a dedicated nurse practitioner to provide WCCs at acute visits. Data were collected for 1 year after full implementation.
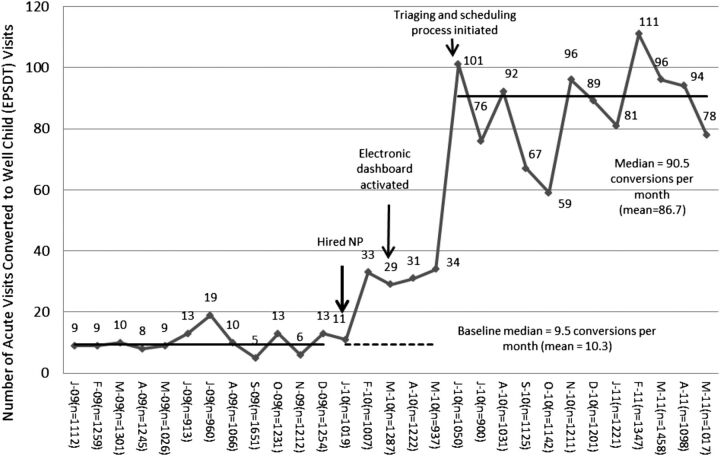
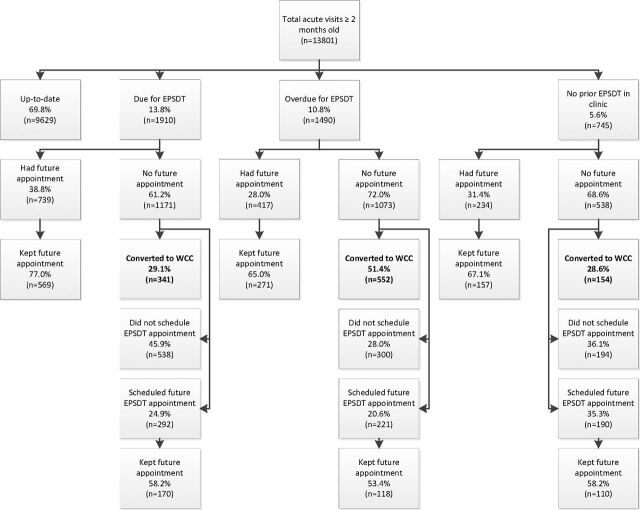
Results: At baseline, 10.3 acute visits per month were converted to WCCs. After intervention, 86.7 acute visits per month were converted. Of 13801 acute visits during the project, 31.2% were not up-to-date. Of those overdue for WCCs, 51.4% (n = 552) were converted to a WCC in addition to the acute visit. Including all patients who were not up-to-date, a total of 1047 acute visits (7.6% of all acute visits) were converted to comprehensive WCCs. Deferring needed WCCs at acute visits resulted in few patients who scheduled or completed future WCC visits.
Conclusions: Implementation of interventions focused on people-process-technology significantly increased WCCs at acute visits within a feasible and practical model that may be replicated at other academic general pediatrics practices.
Conflict of interest statement
Figures

References
-
- Centers for Medicare and Medicaid Services. Early and periodic screening diagnosis & treatment. Available at: www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Benefits/Ea.... Accessed January 17, 2012
-
- Maternal and Child Health Bureau. EPSDT & Title V collaboration to improve child health. Available at: mchb.hrsa.gov/epsdt/index.html. Accessed January 17, 2012
-
- Peters CP . EPSDT: Medicaid’s critical but controversial benefits program for children. NHPF Issue Brief. 2006; (819):1–24 - PubMed
-
- Pittard WB III , Laditka JN , Laditka SB . Early and periodic screening, diagnosis, and treatment and infant health outcomes in Medicaid-insured infants in South Carolina. J Pediatr. 2007;151(4):414–418 - PubMed
-
- Hakim RB , Bye BV . Effectiveness of compliance with pediatric preventive care guidelines among Medicaid beneficiaries. Pediatrics. 2001;108(1):90–97 - PubMed
