

Weight loss and dropout during a commercial weight-loss program including a very-low-calorie diet, a low-calorie diet, or restricted normal food: observational cohort study
- PMID: 22990030
- PMCID: PMC3471207
- DOI: 10.3945/ajcn.112.038265
Weight loss and dropout during a commercial weight-loss program including a very-low-calorie diet, a low-calorie diet, or restricted normal food: observational cohort study
Abstract
Background: The effectiveness of commercial weight-loss programs consisting of very-low-calorie diets (VLCDs) and low-calorie diets (LCDs) is unclear.
Objective: The aim of the study was to quantify weight loss and dropout during a commercial weight-loss program in Sweden (Itrim; cost: $1300/€1000; all participants paid their own fee).
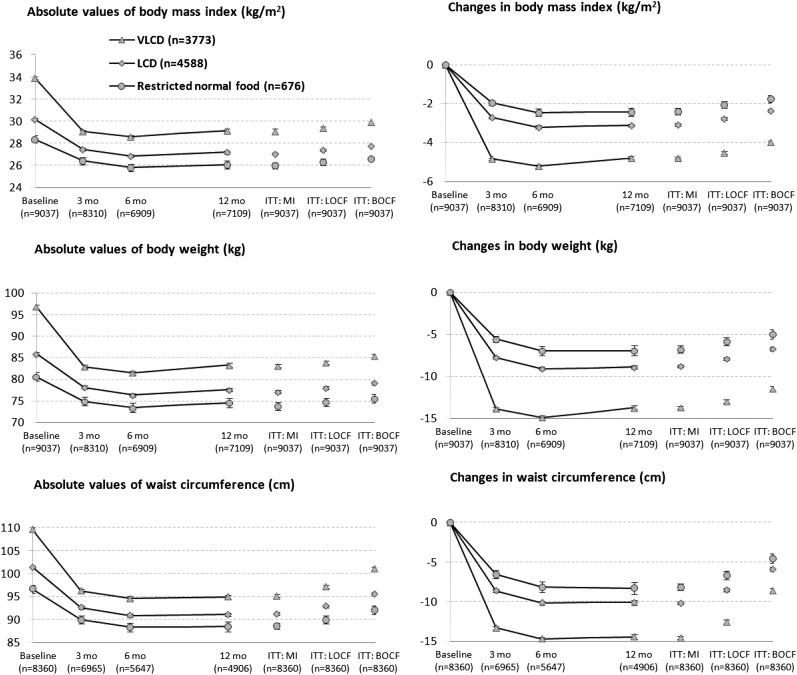
Design: This observational cohort study linked commercial weight-loss data with National Health Care Registers. Weight loss was induced with a 500-kcal liquid-formula VLCD [n = 3773; BMI (in kg/m(2)): 34 ± 5 (mean ± SD); 80% women; 45 ± 12 y of age (mean ± SD)], a 1200-1500-kcal formula and food-combination LCD (n = 4588; BMI: 30 ± 4; 86% women; 50 ± 11 y of age), and a 1500-1800-kcal/d restricted normal-food diet (n = 676; BMI: 29 ± 5; 81% women; 51 ± 12 y of age). Maintenance strategies included exercise and a calorie-restricted diet. Weight loss was analyzed by using an intention-to-treat analysis (baseline substitution).
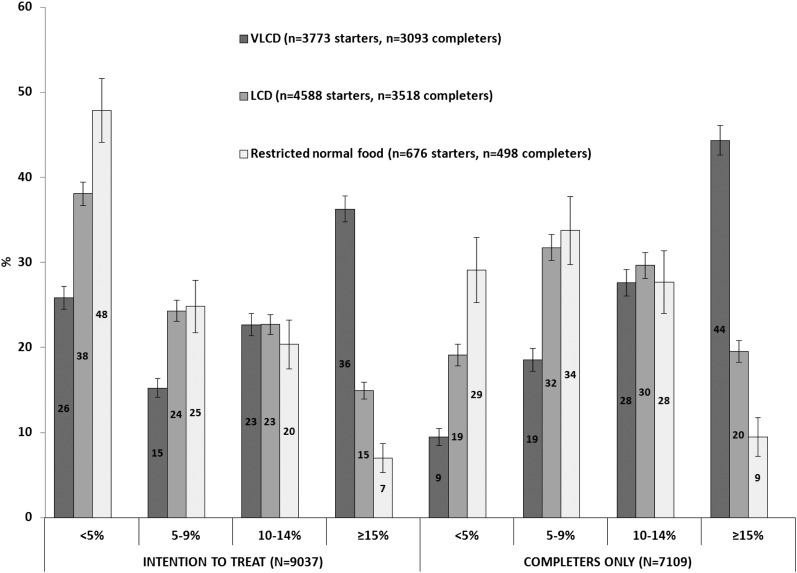
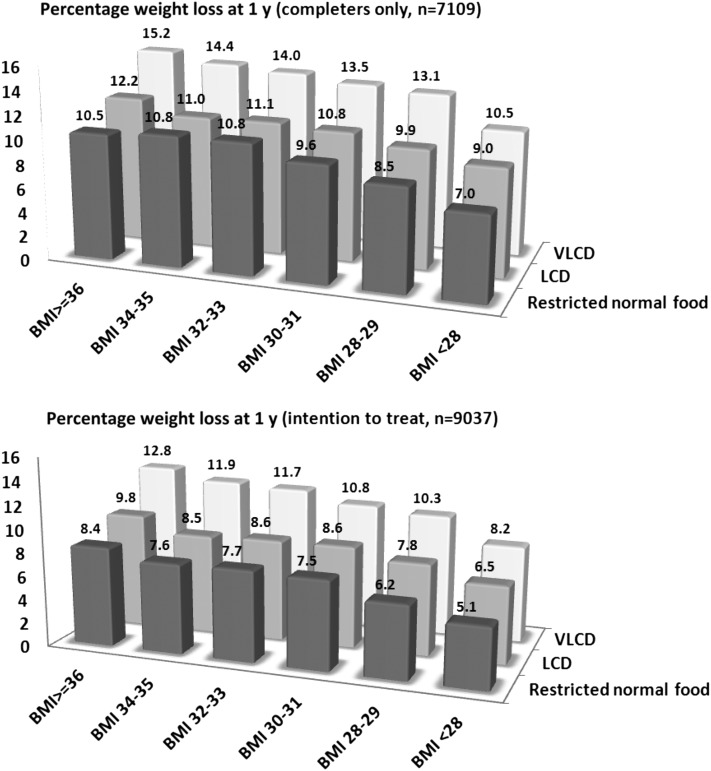
Results: After 1 y, mean (±SD) weight changes were -11.4 ± 9.1 kg with the VLCD (18% dropout), -6.8 ± 6.4 kg with the LCD (23% dropout), and -5.1 ± 5.9 kg with the restricted normal-food diet (26% dropout). In an adjusted analysis, the VLCD group lost 2.8 kg (95% CI: 2.5, 3.2) and 3.8 kg (95% CI: 3.2, 4.5) more than did the LCD and restricted normal-food groups, respectively. A high baseline BMI and rapid initial weight loss were both independently associated with greater 1-y weight loss (P < 0.001). Younger age and low initial weight loss predicted an increased dropout rate (P < 0.001). Treatment of depression (OR: 1.4; 95% CI: 1.1, 1.9) and psychosis (OR: 2.6; 95% CI: 1.1, 6.3) were associated with an increased dropout rate in the VLCD group.
Conclusion: A commercial weight-loss program, particularly one using a VLCD, was effective at reducing body weight in self-selected, self-paying adults.
Figures
Comment in
-
Weight of the nation: moving forward, reversing the trend using medical care.Am J Clin Nutr. 2012 Nov;96(5):949-50. doi: 10.3945/ajcn.112.049643. Epub 2012 Oct 3. Am J Clin Nutr. 2012. PMID: 23034956 Free PMC article. No abstract available.
References
-
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA 2010;303:235–41 - PubMed
-
- Finucane MM, Stevens GA, Cowan MJ, Danaei G, Lin JK, Paciorek CJ, Singh GM, Gutierrez HR, Lu Y, Bahalim AN, et al. National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet 2011;377:557–67 - PMC - PubMed
-
- Adams TD, Gress RE, Smith SC, Halverson RC, Simper SC, Rosamond WD, Lamonte MJ, Stroup AM, Hunt SC. Long-term mortality after gastric bypass surgery. N Engl J Med 2007;357:753–61 - PubMed
-
- Sjöström L, Lindroos AK, Peltonen M, Torgerson J, Bouchard C, Carlsson B, Dahlgren S, Larsson B, Narbro K, Sjostrom CD, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med 2004;351:2683–93 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
