

Clinical characteristics of a cohort of 244 patients with congenital adrenal hyperplasia
- PMID: 22990093
- PMCID: PMC3513542
- DOI: 10.1210/jc.2012-2102
Clinical characteristics of a cohort of 244 patients with congenital adrenal hyperplasia
Abstract
Context: Patients with congenital adrenal hyperplasia (CAH) often suffer from long-term complications secondary to chronic glucocorticoid therapy and suboptimal treatment regimens.
Objective: The aim of the study was to describe clinical characteristics of a large cohort of pediatric and adult CAH patients.
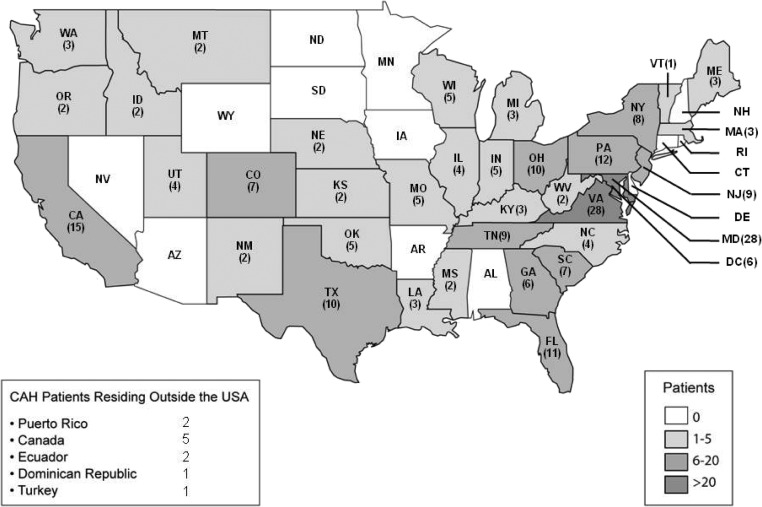
Design and setting: We conducted a cross-sectional study of 244 CAH patients [183 classic, 61 nonclassic (NC)] included in a Natural History Study at the National Institutes of Health.
Main outcome measure(s): Outcome variables of interest were height sd score, obesity, hypertensive blood pressure (BP), insulin resistance, metabolic syndrome, bone mineral density, hirsutism (females), and testicular adrenal rest (TART).
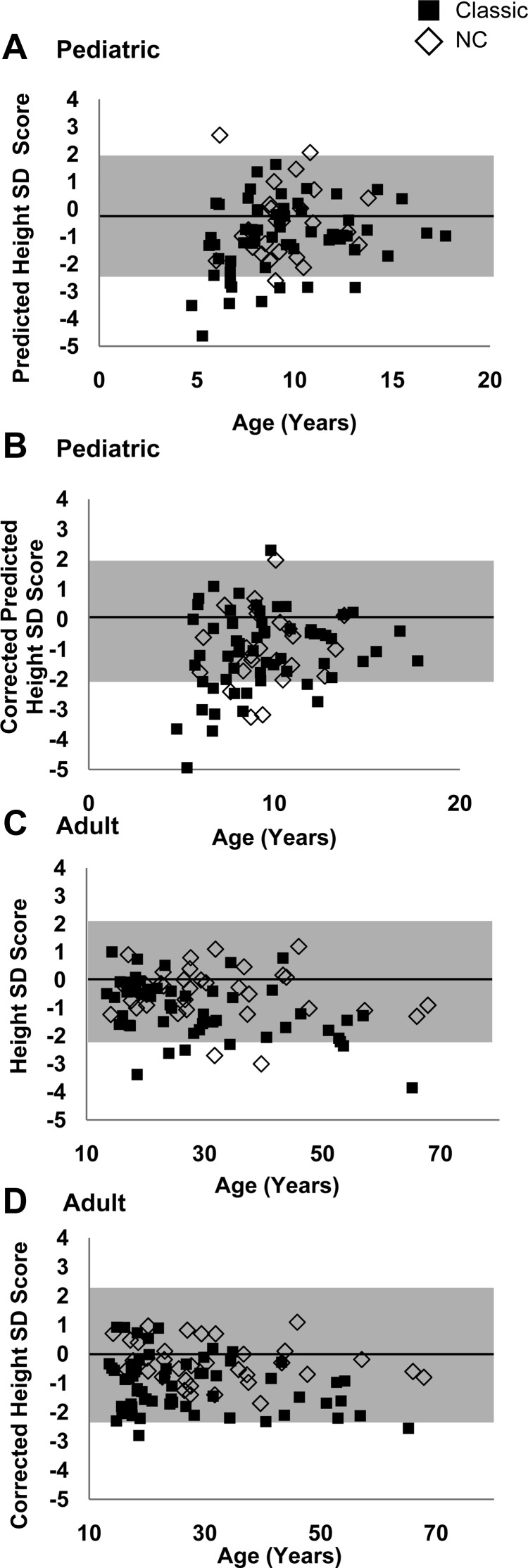
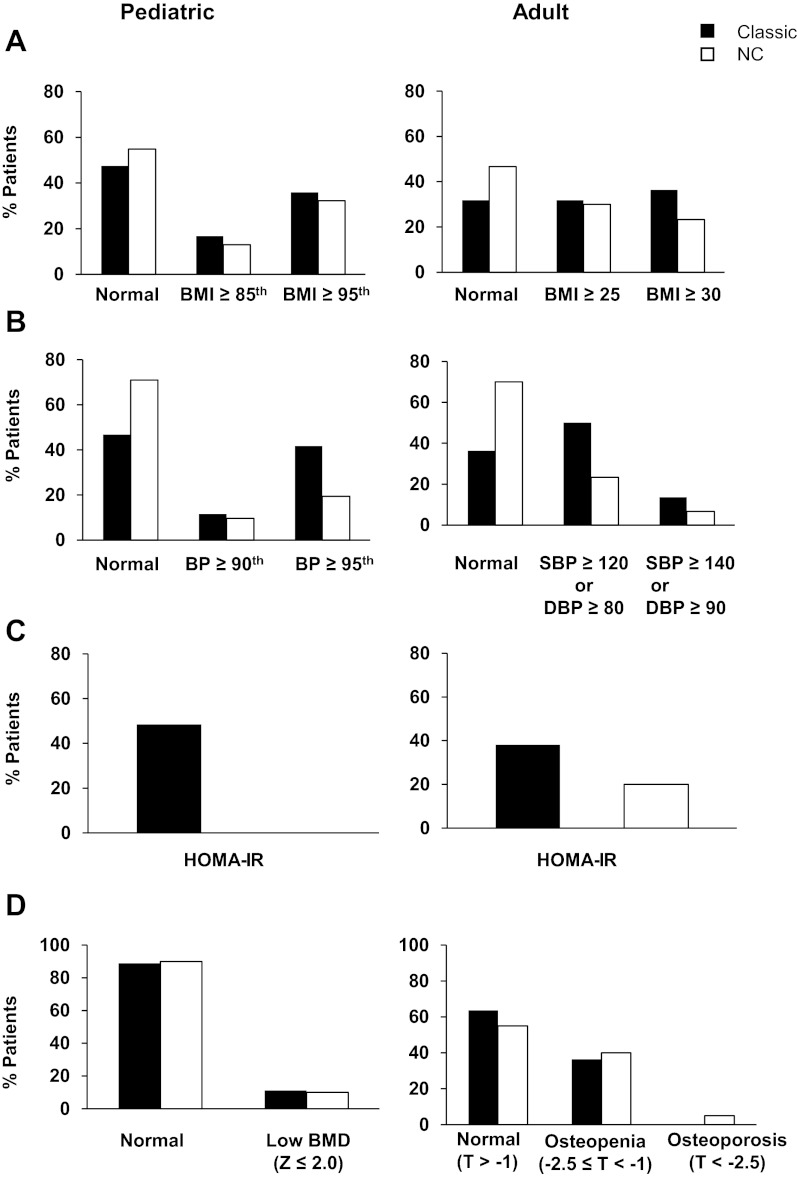
Results: The majority had elevated or suppressed androgens, with varied treatment regimens. Mean adult height SD score was -1.0 ± 1.1 for classic vs. -0.4 ± 0.9 for NC patients (P = 0.015). Obesity was present in approximately one third of patients, across phenotypes. Elevated BP was more common in classic than NC patients (P ≤ 0.01); pediatric hypertensive BP was associated with suppressed plasma renin activity (P = 0.001). Insulin resistance was common in classic children (27%) and adults (38% classic, 20% NC); 18% of adults had metabolic syndrome. The majority (61%) had low vitamin D; 37% of adults had low bone mineral density. Hirsutism was common (32% classic; 59% NC women). TART was found in classic males (33% boys; 44% men).
Conclusions: Poor hormonal control and adverse outcomes are common in CAH, necessitating new treatments. Routine monitoring of classic children should include measuring BP and plasma renin activity. Osteoporosis prophylaxis and TART screening should begin during childhood. A longitudinal study is under way.
Trial registration: ClinicalTrials.gov NCT00250159.
Figures

References
-
- Merke DP, Bornstein SR. 2005. Congenital adrenal hyperplasia. Lancet 365:2125–2136 - PubMed
-
- Speiser PW, Azziz R, Baskin LS, Ghizzoni L, Hensle TW, Merke DP, Meyer-Bahlburg HF, Miller WL, Montori VM, Oberfield SE, Ritzen M, White PC. 2010. Congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 95:4133–4160 - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
