

Exercise dose and diabetes risk in overweight and obese children: a randomized controlled trial
- PMID: 22990269
- PMCID: PMC3487697
- DOI: 10.1001/2012.jama.10762
Exercise dose and diabetes risk in overweight and obese children: a randomized controlled trial
Abstract
Context: Pediatric studies have shown that aerobic exercise reduces metabolic risk, but dose-response information is not available.
Objectives: To test the effect of different doses of aerobic training on insulin resistance, fatness, visceral fat, and fitness in overweight, sedentary children and to test moderation by sex and race.
Design, setting, and participants: Randomized controlled efficacy trial conducted from 2003 through 2007 in which 222 overweight or obese sedentary children (mean age, 9.4 years; 42% male; 58% black) were recruited from 15 public schools in the Augusta, Georgia, area.
Intervention: Children were randomly assigned to low-dose (20 min/d; n = 71) or high-dose (40 min/d; n = 73) aerobic training (5 d/wk; mean duration, 13 [SD, 1.6] weeks) or a control condition (usual physical activity; n = 78).
Main outcome measures: The prespecified primary outcomes were postintervention type 2 diabetes risk assessed by insulin area under the curve (AUC) from an oral glucose tolerance test, aerobic fitness (peak oxygen consumption [VO2]), percent body fat via dual-energy x-ray absorptiometry, and visceral fat via magnetic resonance, analyzed by intention to treat.
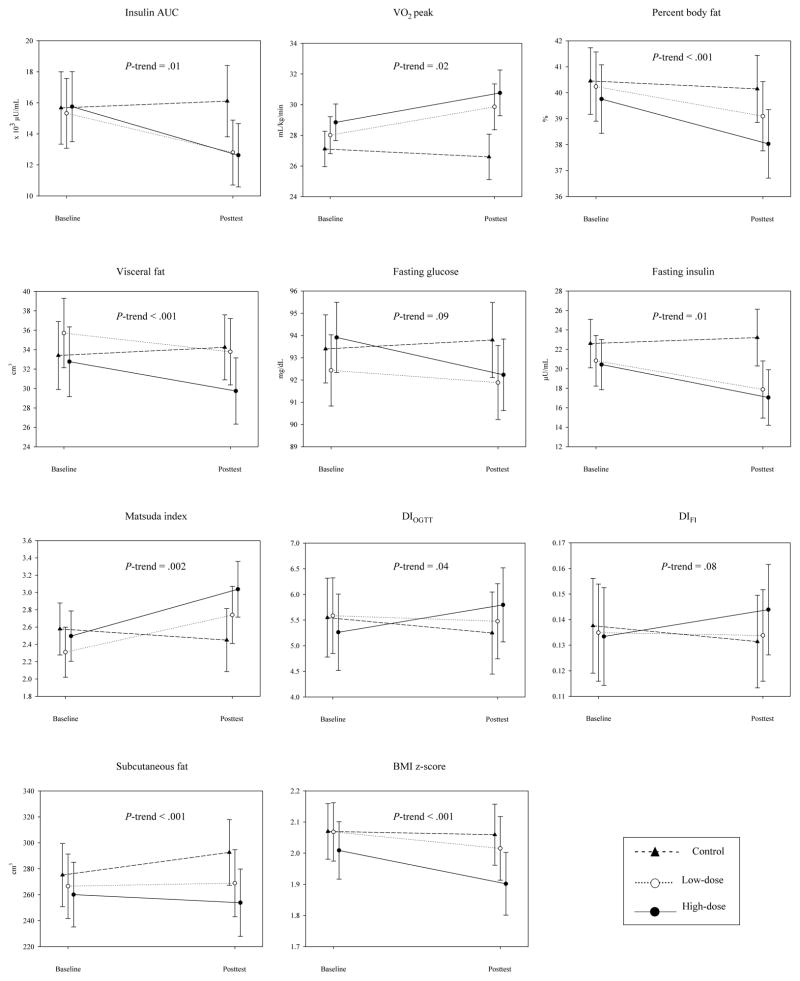
Results: The study had 94% retention (n = 209). Most children (85%) were obese. At baseline, mean body mass index was 26 (SD, 4.4). Reductions in insulin AUC were larger in the high-dose group (adjusted mean difference, -3.56 [95% CI, -6.26 to -0.85] × 10(3) μU/mL; P = .01) and the low-dose group (adjusted mean difference, -2.96 [95% CI, -5.69 to -0.22] × 10(3) μU/mL; P = .03) than the control group. Dose-response trends were also observed for body fat (adjusted mean difference, -1.4% [95% CI, -2.2% to -0.7%]; P < .001 and -0.8% [95% CI, -1.6% to -0.07%]; P = .03) and visceral fat (adjusted mean difference, -3.9 cm3 [95% CI, -6.0 to -1.7 cm3]; P < .001 and -2.8 cm3 [95% CI, -4.9 to -0.6 cm3]; P = .01) in the high- and low-dose vs control groups, respectively. Effects in the high- and low-dose groups vs control were similar for fitness (adjusted mean difference in peak VO2, 2.4 [95% CI, 0.4-4.5] mL/kg/min; P = .02 and 2.4 [95% CI, 0.3-4.5] mL/kg/min; P = .03, respectively). High- vs low-dose group effects were similar for these outcomes. There was no moderation by sex or race.
Conclusion: In this trial, after 13 weeks, 20 or 40 min/d of aerobic training improved fitness and demonstrated dose-response benefits for insulin resistance and general and visceral adiposity in sedentary overweight or obese children, regardless of sex or race.
Trial registration: clinicaltrials.gov Identifier: NCT00108901.
Conflict of interest statement
Figures

Comment in
-
Randomised trial of exercise dose in children reduces diabetes risk (as measured by insulin resistance) in both 20-min and 40-min doses.Evid Based Med. 2013 Aug;18(4):147-8. doi: 10.1136/eb-2012-101092. Epub 2012 Dec 4. Evid Based Med. 2013. PMID: 23213116 No abstract available.
-
Exercise for overweight children and diabetes risk.JAMA. 2013 Jan 9;309(2):133. doi: 10.1001/jama.2012.148056. JAMA. 2013. PMID: 23299592 No abstract available.
-
Exercise for overweight children and diabetes risk--reply.JAMA. 2013 Jan 9;309(2):133-4. doi: 10.1001/jama.2012.148059. JAMA. 2013. PMID: 23299593 Free PMC article. No abstract available.
-
Exercise demonstrates a dose-response effect on insulin resistance, fatness, and visceral fat.J Pediatr. 2013 Mar;162(3):649-50. doi: 10.1016/j.jpeds.2012.12.059. J Pediatr. 2013. PMID: 23438919 Free PMC article. No abstract available.
References
-
- Strauss RS, Pollack HA. Epidemic increase in childhood overweight, 1986–1998. JAMA. 2001 Dec 12;286(22):2845–2848. - PubMed
-
- Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007–2008. JAMA. 2010 Jan 20;303(3):242–249. - PubMed
-
- Davis CL, Kapuku G, Snieder H, Kumar M, Treiber FA. Insulin resistance syndrome and left ventricular mass in healthy young people. Am J Med Sci. 2002 Aug;324(2):72–75. - PubMed
-
- Davis CL, Flickinger B, Moore D, Bassali R, Domel Baxter S, Yin Z. Prevalence of cardiovascular risk factors in schoolchildren in a rural Georgia community. Am J Med Sci. 2005 Aug;330(2):53–59. - PubMed
-
- Pinhas-Hamiel O, Dolan LM, Daniels SR, Standiford D, Khoury PR, Zeitler P. Increased incidence of non-insulin-dependent diabetes mellitus among adolescents. J Pediatr. 1996;128(5 Pt 1):608–615. - PubMed
