

Postoperative pharyngocutaneous fistula: treated by sternocleidomastoid flap repair and cricopharyngeus myotomy
- PMID: 22990605
- PMCID: PMC3540315
- DOI: 10.1007/s00586-012-2451-4
Postoperative pharyngocutaneous fistula: treated by sternocleidomastoid flap repair and cricopharyngeus myotomy
Abstract
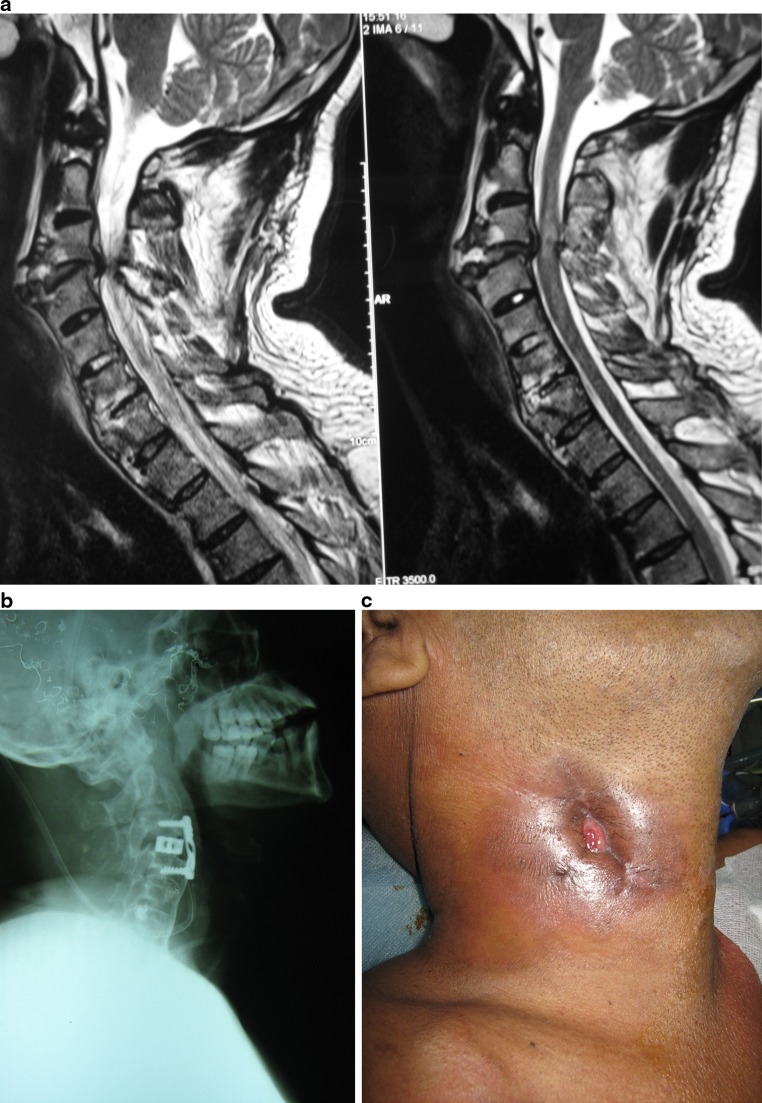
Introduction: Pharyngoesophagocutaneous fistula (PEF) is one of the rare but serious complications of antero-lateral approach to cervical spine surgery. Because of its rarity, the true incidence of PEF is not clear. But, retrospective analysis of large series of cervical spine surgery reports 0-1.62 % incidence (Cloward in Surg 69:175-182, 1971; Elerkay et al. in J Neurosurg Spine 90(Suppl 1):35-41, 1999). Proximity to the vertebral column and thin walls makes the upper digestive tract vulnerable to injury in cervical trauma, surgical or nonsurgical. Presentation in early postoperative period is not rare and carries high morbidity and mortality (Jones and Ginsberg in Ann Thorac Surg 53(3):534-543, 1992). Various procedures for these fistulae such as simple closure, muscle flap interposition, esophageal diversion and jejunal interposition are reported. Some authors also advise removal of prosthetic plates and posterior stabilization, besides the repair of fistulae in a staged manner (Orlando et al. in Spine 28(15):E290-E295, 2003).
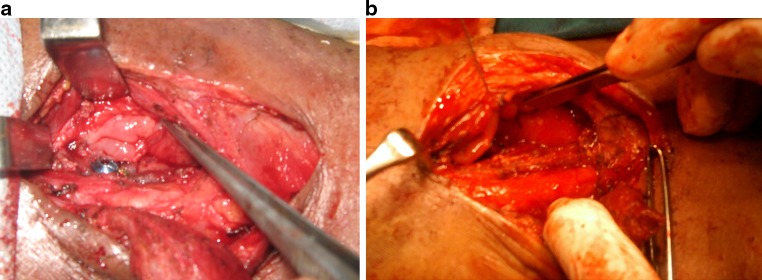
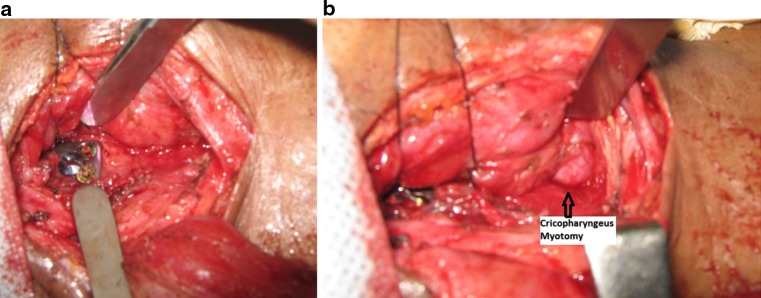
Methods: Two similar cases of pharyngeal fistulae with similar etiology and clinical scenario are presented here, which were managed successfully with initial control of sepsis followed by delayed definitive repair with sternocleidomastoid muscle flap interposition and cricopharyngeus myotomy without removal of prosthetic plates.
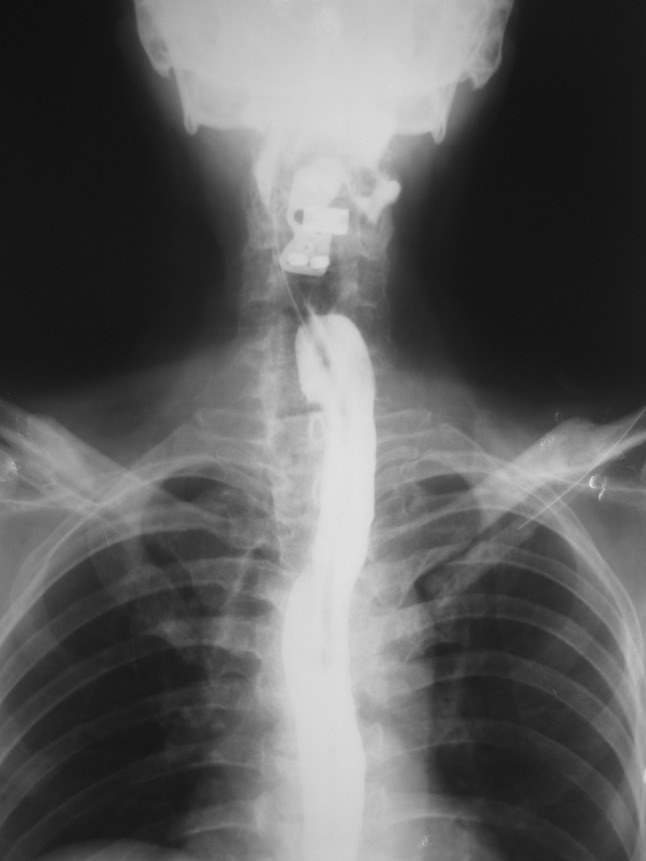
Results: Postoperatively, both patients showed no evidence of any wound complications or collections until the seventh day. A contrast swallow study on seventh day showed no leak following which soft diet was started. Both patients were not having any difficulty in swallowing or aspiration. On 1-year follow-up, both patients were having no difficulty in swallowing, no episodes of aspiration and no recurrence of fistula.
Conclusion: This case series highlights the importance of cricopharyngeus myotomy for treating PEF and the improved results with the prosthesis kept undisturbed.
Figures


Comment in
-
Expert's comment concerning grand rounds case entitled ''postoperative pharyngocutaneous fistula: treated with sternocleidomastoid flap repair and cricopharyngeus myotomy'' (by V.A. Iyoob).Eur Spine J. 2013 Jan;22(1):113-5. doi: 10.1007/s00586-012-2453-2. Epub 2012 Sep 22. Eur Spine J. 2013. PMID: 23001379 Free PMC article.
Similar articles
-
Expert's comment concerning grand rounds case entitled ''postoperative pharyngocutaneous fistula: treated with sternocleidomastoid flap repair and cricopharyngeus myotomy'' (by V.A. Iyoob).Eur Spine J. 2013 Jan;22(1):113-5. doi: 10.1007/s00586-012-2453-2. Epub 2012 Sep 22. Eur Spine J. 2013. PMID: 23001379 Free PMC article.
-
Pharyngocutaneous fistula after anterior cervical spine surgery.Eur Spine J. 2009 May;18(5):586-91. doi: 10.1007/s00586-009-0951-7. Epub 2009 Mar 28. Eur Spine J. 2009. PMID: 19330360 Free PMC article.
-
Delayed platysma myocutaneous turnover flap for repair of pharyngocutaneous fistula.Am J Otolaryngol. 2015 Jan-Feb;36(1):93-6. doi: 10.1016/j.amjoto.2014.08.015. Epub 2014 Sep 3. Am J Otolaryngol. 2015. PMID: 25241029
-
[Pharyngo-vertebral fistula with transspinous course to the neck skin due to a cervical spondylodesis - case report and review of the literature].Z Orthop Unfall. 2009 Mar-Apr;147(2):215-9. doi: 10.1055/s-0029-1185410. Epub 2009 Apr 8. Z Orthop Unfall. 2009. PMID: 19358078 Review. German.
-
Free gastro-omental flap reconstruction of the complex, irradiated pharyngeal wound.Head Neck. 1997 Jan;19(1):68-71. doi: 10.1002/(sici)1097-0347(199701)19:1<68::aid-hed13>3.0.co;2-n. Head Neck. 1997. PMID: 9030949 Review.
Cited by
-
Survival Analysis of Patients with Osseous Malignant Vascular Tumors: Results of the Surveillance, Epidemiology, and End Results (SEER) Database from 1973 to 2015.Med Sci Monit. 2019 Jul 25;25:5525-5535. doi: 10.12659/MSM.914950. Med Sci Monit. 2019. PMID: 31344019 Free PMC article.
-
Chronicle of coughed up screws.Med J Armed Forces India. 2016 Dec;72(Suppl 1):S150-S152. doi: 10.1016/j.mjafi.2016.03.015. Epub 2016 May 26. Med J Armed Forces India. 2016. PMID: 28050099 Free PMC article. No abstract available.
-
Pharyngocutaneous Fistula and Horner's Syndrome following Loosening of Locking Screw of Anterior Cervical Plating: A Rare Case Report and Management.Asian J Neurosurg. 2021 Feb 23;16(1):196-199. doi: 10.4103/ajns.AJNS_230_19. eCollection 2021 Jan-Mar. Asian J Neurosurg. 2021. PMID: 34211894 Free PMC article.
-
Expert's comment concerning grand rounds case entitled ''postoperative pharyngocutaneous fistula: treated with sternocleidomastoid flap repair and cricopharyngeus myotomy'' (by V.A. Iyoob).Eur Spine J. 2013 Jan;22(1):113-5. doi: 10.1007/s00586-012-2453-2. Epub 2012 Sep 22. Eur Spine J. 2013. PMID: 23001379 Free PMC article.
-
Sternocleidomastoid flap augmentation of the pharyngeal closure after total laryngectomy.Eur Arch Otorhinolaryngol. 2017 Aug;274(8):3197-3202. doi: 10.1007/s00405-017-4582-z. Epub 2017 May 15. Eur Arch Otorhinolaryngol. 2017. PMID: 28508179
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
