

Nosocomial infections in adult cardiogenic shock patients supported by venoarterial extracorporeal membrane oxygenation
- PMID: 22990851
- PMCID: PMC3888098
- DOI: 10.1093/cid/cis783
Nosocomial infections in adult cardiogenic shock patients supported by venoarterial extracorporeal membrane oxygenation
Abstract
Background: Incidence and impact on adult patients' outcomes of nosocomial infections (NIs) occurring during venoarterial extracorporeal membrane oxygenation (VA-ECMO) support for refractory cardiogenic shock have rarely been described.
Methods: We retrospectively reviewed the charts of a large series of patients who received VA-ECMO in our intensive care unit (ICU) from January 2003 through December 2009. Incidence, types, risk factors, and impact on outcomes of NIs occurring during ECMO support were analyzed.
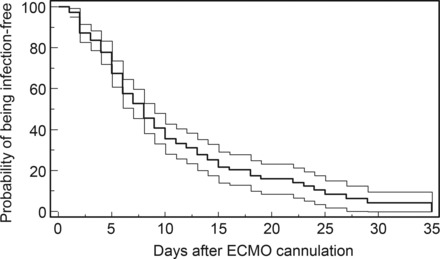
Results: Among 220 patients (49 ± 16 years old, simplified acute physiology score (SAPS) II 61 ± 20) who underwent ECMO support for >48 hours for a total of 2942 ECMO days, 142 (64%) developed NIs. Ventilator-associated pneumonia (VAP), bloodstream infections, cannula infections, and mediastinitis infections occurred in 55%, 18%, 10% and 11% of the patients, respectively. More critical condition at ICU admission, but not antibiotics at the time of ECMO cannulation, was associated with subsequently developing NIs (hazard ratio, 0.73; 95% confidence interval [CI], .50-1.05; P = .09). Infected patients had longer durations of mechanical ventilation, ECMO support, and hospital stays. Independent predictors of death were infection with severe sepsis or septic shock (odds ratio, 1.93; 95% CI, 1.26-2.94; P = .002) and SAPS II, whereas immunosuppression and myocarditis as the reason for ECMO support were associated with better outcomes.
Conclusions: Cardiogenic shock patients who received the latest generation VA-ECMO still had a high risk of developing NIs, particularly VAP. Strategies aimed at preventing these infections may improve the outcomes of these critically ill patients.
Figures
References
-
- Chen YS, Chao A, Yu HY, et al. Analysis and results of prolonged resuscitation in cardiac arrest patients rescued by extracorporeal membrane oxygenation. J Am Coll Cardiol. 2003;41:197–203. - PubMed
-
- Magovern GJ, Jr., Simpson KA. Extracorporeal membrane oxygenation for adult cardiac support: the Allegheny experience. Ann Thorac Surg. 1999;68:655–61. - PubMed
-
- Smedira NG, Moazami N, Golding CM, et al. Clinical experience with 202 adults receiving extracorporeal membrane oxygenation for cardiac failure: survival at five years. J Thorac Cardiovasc Surg. 2001;122:92–102. - PubMed
-
- Chen JS, Ko WJ, Yu HY, et al. Analysis of the outcome for patients experiencing myocardial infarction and cardiopulmonary resuscitation refractory to conventional therapies necessitating extracorporeal life support rescue. Crit Care Med. 2006;34:950–7. - PubMed
-
- Combes A, Leprince P, Luyt CE, et al. Outcomes and long-term quality-of-life of patients supported by extracorporeal membrane oxygenation for refractory cardiogenic shock. Crit Care Med. 2008;36:1404–11. - PubMed
