

An economic evaluation: Simulation of the cost-effectiveness and cost-utility of universal prevention strategies against osteoporosis-related fractures
- PMID: 22991210
- PMCID: PMC3580046
- DOI: 10.1002/jbmr.1758
An economic evaluation: Simulation of the cost-effectiveness and cost-utility of universal prevention strategies against osteoporosis-related fractures
Abstract
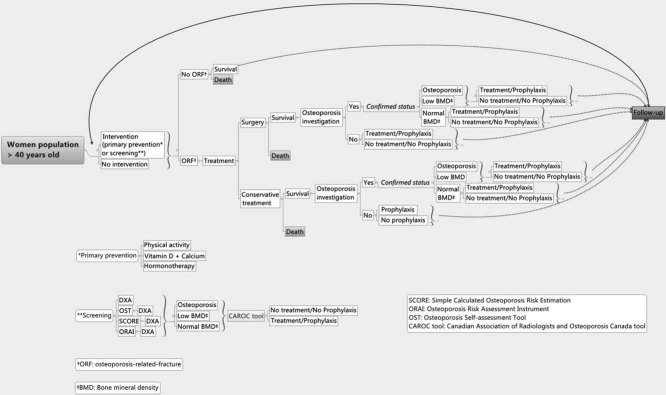
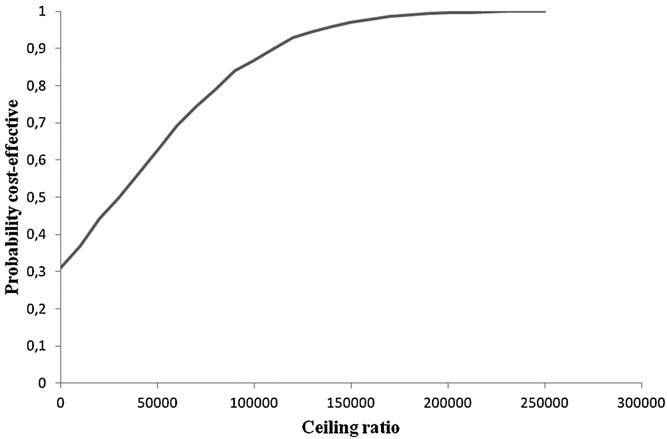
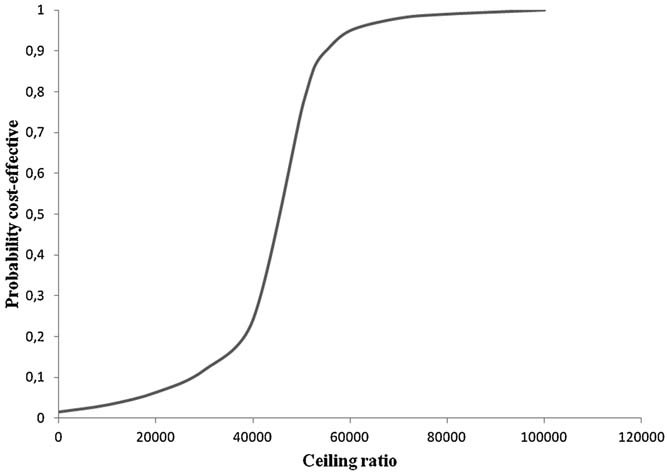
A patient-level Markov decision model was used to simulate a virtual cohort of 500,000 women 40 years old and over, in relation to osteoporosis-related hip, clinical vertebral, and wrist bone fractures events. Sixteen different screening options of three main scenario groups were compared: (1) the status quo (no specific national prevention program); (2) a universal primary prevention program; and (3) a universal screening and treatment program based on the 10-year absolute risk of fracture. The outcomes measured were total directs costs from the perspective of the public health care system, number of fractures, and quality-adjusted life-years (QALYs). Results show that an option consisting of a program promoting physical activity and treatment if a fracture occurs is the most cost-effective (CE) (cost/fracture averted) alternative and also the only cost saving one, especially for women 40 to 64 years old. In women who are 65 years and over, bone mineral density (BMD)-based screening and treatment based on the 10-year absolute fracture risk calculated using a Canadian Association of Radiologists and Osteoporosis Canada (CAROC) tool is the best next alternative. In terms of cost-utility (CU), results were similar. For women less than 65 years old, a program promoting physical activity emerged as cost-saving but BMD-based screening with pharmacological treatment also emerged as an interesting alternative. In conclusion, a program promoting physical activity is the most CE and CU option for women 40 to 64 years old. BMD screening and pharmacological treatment might be considered a reasonable alternative for women 65 years old and over because at a healthcare capacity of $50,000 Canadian dollars ($CAD) for each additional fracture averted or for one QALY gained its probabilities of cost-effectiveness compared to the program promoting physical activity are 63% and 75%, respectively, which could be considered socially acceptable. Consideration of the indirect costs could change these findings.
Copyright © 2013 American Society for Bone and Mineral Research.
Figures
Similar articles
-
Cost-effectiveness of a multifaceted intervention to improve quality of osteoporosis care after wrist fracture.Osteoporos Int. 2011 Jun;22(6):1799-808. doi: 10.1007/s00198-010-1412-1. Epub 2010 Sep 29. Osteoporos Int. 2011. PMID: 20878389 Clinical Trial.
-
Economic evaluation of a population-based osteoporosis intervention for outpatients with non-traumatic non-hip fractures: the "Catch a Break" 1i [type C] FLS.Osteoporos Int. 2017 Jun;28(6):1965-1977. doi: 10.1007/s00198-017-3986-3. Epub 2017 Mar 9. Osteoporos Int. 2017. PMID: 28275838 Free PMC article.
-
Cost-effectiveness of a fracture liaison service--a real-world evaluation after 6 years of service provision.Osteoporos Int. 2016 Jan;27(1):231-40. doi: 10.1007/s00198-015-3280-1. Epub 2015 Aug 15. Osteoporos Int. 2016. PMID: 26275439
-
Economic impact and cost-effectiveness of fracture liaison services: a systematic review of the literature.Osteoporos Int. 2018 Jun;29(6):1227-1242. doi: 10.1007/s00198-018-4411-2. Epub 2018 Feb 19. Osteoporos Int. 2018. PMID: 29460102
-
The cost effectiveness of bisphosphonates for the prevention and treatment of osteoporosis: a structured review of the literature.Pharmacoeconomics. 2007;25(11):913-33. doi: 10.2165/00019053-200725110-00003. Pharmacoeconomics. 2007. PMID: 17960951 Review.
Cited by
-
Redefining the Economics of Geriatric Orthopedics.Geriatr Orthop Surg Rehabil. 2014 Dec;5(4):200-6. doi: 10.1177/2151458514543002. Geriatr Orthop Surg Rehabil. 2014. PMID: 26246943 Free PMC article.
-
Protocol for the models of primary osteoporosis screening in men (MOPS) cluster randomized trial.Contemp Clin Trials. 2022 Jan;112:106634. doi: 10.1016/j.cct.2021.106634. Epub 2021 Nov 27. Contemp Clin Trials. 2022. PMID: 34844000 Free PMC article.
-
Economic evaluation of vitamin D and calcium food fortification for fracture prevention in Germany.Public Health Nutr. 2017 Jul;20(10):1874-1883. doi: 10.1017/S1368980015003171. Epub 2015 Nov 16. Public Health Nutr. 2017. PMID: 26568196 Free PMC article.
-
Construction of a predictive model for osteoporosis risk in men: using the IOF 1-min osteoporosis test.J Orthop Surg Res. 2023 Oct 11;18(1):770. doi: 10.1186/s13018-023-04266-7. J Orthop Surg Res. 2023. PMID: 37821993 Free PMC article.
-
A model-based cost-effectiveness analysis of osteoporosis screening and treatment strategy for postmenopausal Japanese women.Osteoporos Int. 2017 Feb;28(2):643-652. doi: 10.1007/s00198-016-3782-5. Epub 2016 Oct 14. Osteoporos Int. 2017. PMID: 27743068
References
-
- Cheung AM, Feig DS, Kapral M, Diaz-Granados N, Dodin S. Canadian Task Force on Preventive Health Care. Prevention of osteoporosis and osteoporotic fractures in postmenopausal women: recommendation statement from the Canadian Task Force on Preventive Health Care. CMAJ. 2004;170(11):1665–7. - PMC - PubMed
-
- Melton LJ, 3rd, Chrischilles EA, Cooper C, Lane AW, Riggs BL. Perspective. How many women have osteoporosis? J Bone Miner Res. 1992;7(9):1005–10. - PubMed
-
- Agence d'évaluation des technologies et des modes d'intervention en santé (AETMIS) Rapport préparé par Michel Rossignol et collaborateurs. (AÉTMIS 04-1RF) Montréal; Canada: AÉTMIS; 2001. pp. ix–68. L'ostéoporose et les fractures chez les personnes de 65 ans et plus: recommandations pour un cadre intégré d'intervention au Québec.
-
- Papaioannou A, Morin S, Cheung AM, Atkinson S, Brown JP, Feldman S, Hanley DA, Hodsman A, Jamal SA, Kaiser SM, Kvern B, Siminoski K, Leslie WD. Scientific Advisory Council of Osteoporosis Canada. 2010 Clinical practice guidelines for the diagnosis and management of osteoporosis in Canada: summary. CMAJ. 2010;182(17):1864–73. - PMC - PubMed
-
- Stevenson M, Jones ML, De Nigris E, Brewer N, Davis S, Oakley J. A systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosis. Health Technol Assess. 2005;9(22):1–160. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
