

Biomarkers of HPV in head and neck squamous cell carcinoma
- PMID: 22991304
- PMCID: PMC3463756
- DOI: 10.1158/0008-5472.CAN-11-3277
Biomarkers of HPV in head and neck squamous cell carcinoma
Abstract
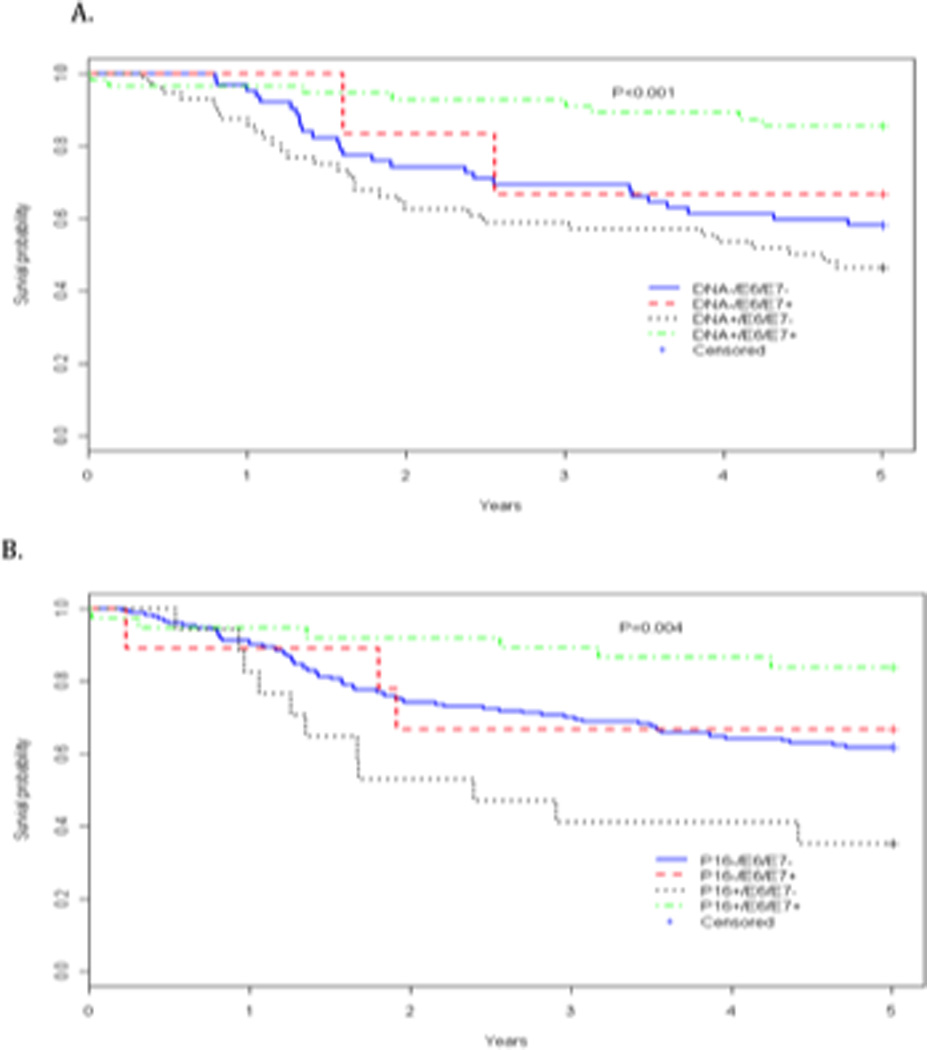
Human papillomavirus (HPV) is an accepted cause of head and neck squamous cell carcinoma (HNSCC), and patients with HPV-associated HNSCC have a favorable prognosis. Currently, there is no general guidance on the most appropriate biomarkers for clinical assessment of HPV in these malignancies. We compared PCR-based and serologic HPV assays, as well as p16 immunohistochemistry, individually and in combination in a single population-based study to assess their associations with overall survival among patients with HNSCC, and thus their potential value as biomarkers. HPV16 serology was determined for 488 patients; immunohistochemical detection of p16 expression in tumors was conducted in a subset of 233 cases, and PCR-based methods to assess the presence of HPV16 DNA in a subset of 179 cases of tumors. Considering each biomarker individually in the subset of patients studied for all endpoints, seropositivity for the E6 and E7 proteins was significantly associated with enhanced all-cause survival in oropharyngeal disease [HR(E6/E7+) = 0.1, 95% confidence interval (CI) = 0.02-0.3]. Neither the presence of HPV16 DNA nor p16 immunostaining was associated with significant enhanced overall survival in oropharyngeal disease (HR(DNA) = 0.9, 95% CI = 0.3-2.9; HR(p16) = 0.3, 95% CI = 0.1-1.1). However, the combination of HPV-positive DNA and E6 or E7 serology was associated with enhanced overall survival in oropharyngeal disease (HR(DNA+/E6/E7+) = 0.1, 95% CI = 0.02-1.0), whereas E6/E7 seronegative patients with evidence of HPV in tumor DNA did not show any evidence of favorable survival (HR(DNA+/E6-/E7-) = 3.4, 95% CI = 0.6-18.1). Furthermore, patients with p16 staining and E6 or E7 seropositivity had favorable survival from oropharyngeal disease (HR(p16+/E6/E7+) = 0.1, 95% CI = 0.02-0.4), whereas patients who were p16 positive and E6/E7 seronegative had significantly increased hazard of all causes of death (HR(p16+/E6-/E7-) = 3.1, 95% CI = 1.2-7.7). A stronger association of HPV presence with prognosis (assessed by all-cause survival) is observed when "HPV-associated" HNSCC is defined using tumor status (HPV DNA status or P16) and HPV E6/E7 serology in combination rather using tumor HPV status alone.
©2012 AACR.
Conflict of interest statement
Figures

Comment in
-
Biomarkers of HPV infection in oropharyngeal carcinomas: can we find simplicity in the puzzle of complexity?Cancer Res. 2012 Oct 1;72(19):4896-8. doi: 10.1158/0008-5472.CAN-12-3285. Epub 2012 Sep 18. Cancer Res. 2012. PMID: 22991303 No abstract available.
References
-
- Pintos J, et al. Human papillomavirus infection and oral cancer: a case-control study in Montreal, Canada. Oral Oncol. 2008;44(3):242–250. - PubMed
-
- Smith EM, et al. Age, sexual behavior and human papillomavirus infection in oral cavity and oropharyngeal cancers. Int J Cancer. 2004;108(5):766–772. - PubMed
-
- Zumbach K, et al. Antibodies against oncoproteins E6 and E7 of human papillomavirus types 16 and 18 in patients with head-and-neck squamous-cell carcinoma. Int J Cancer. 2000;85(6):815–818. - PubMed
-
- Smith EM, et al. Human papillomavirus seropositivity and risks of head and neck cancer. Int J Cancer. 2007;120(4):825–832. - PubMed
-
- Santin AD, et al. Radiation-enhanced expression of E6/E7 transforming oncogenes of human papillomavirus-16 in human cervical carcinoma. Cancer. 1998;83(11):2346–2352. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
