

Clinical significance of the genetic landscape of pancreatic cancer and implications for identification of potential long-term survivors
- PMID: 22991414
- PMCID: PMC3500447
- DOI: 10.1158/1078-0432.CCR-12-1215
Clinical significance of the genetic landscape of pancreatic cancer and implications for identification of potential long-term survivors
Abstract
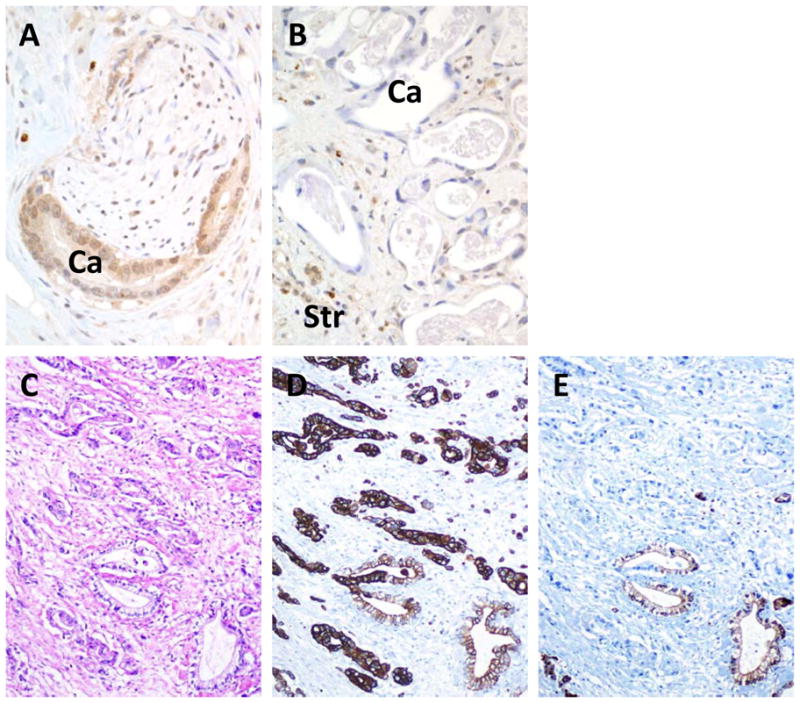
Purpose: Genetic alterations of KRAS, CDKN2A, TP53, and SMAD4 are the most frequent events in pancreatic cancer. We determined the extent to which these 4 alterations are coexistent in the same carcinoma, and their impact on patient outcome.
Experimental design: Pancreatic cancer patients who underwent an autopsy were studied (n = 79). Matched primary and metastasis tissues were evaluated for intragenic mutations in KRAS, CDKN2A, and TP53 and immunolabeled for CDKN2A, TP53, and SMAD4 protein products. The number of altered driver genes in each carcinoma was correlated to clinicopathologic features. Kaplan-Meier estimates were used to determine median disease free and overall survival, and a Cox proportional hazards model used to compare risk factors.
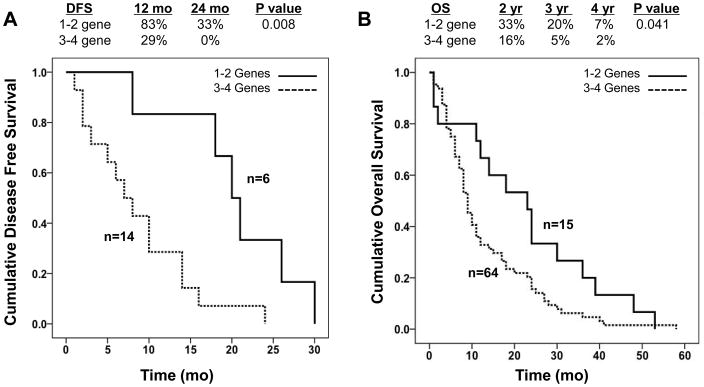
Results: The number of genetically altered driver genes in a carcinoma was variable, with only 29 patients (37%) having an alteration in all 4 genes analyzed. The number of altered driver genes was significantly correlated with disease free survival (P = 0.008), overall survival (P = 0.041), and metastatic burden at autopsy (P = 0.002). On multivariate analysis, the number of driver gene alterations in a pancreatic carcinoma remained independently associated with overall survival (P = 0.046). Carcinomas with only 1 to 2 driver alterations were enriched for those patients with the longest survival (median 23 months, range 1 to 53).
Conclusions: Determinations of the status of the 4 major driver genes in pancreatic cancer, and specifically the extent to which they are coexistent in an individual patients cancer, provides distinct information regarding disease progression and survival that is independent of clinical stage and treatment status.
©2012 AACR.
Conflict of interest statement
The authors have no financial conflicts of interest related to this work.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62(1):10–29. - PubMed
-
- Balakrishnan A, Bleeker FE, Lamba S, Rodolfo M, Daniotti M, Scarpa A, et al. Novel somatic and germline mutations in cancer candidate genes in glioblastoma, melanoma, and pancreatic carcinoma. Cancer Res. 2007;67(8):3545–50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
