

Design and rationale of the MR-INFORM study: stress perfusion cardiovascular magnetic resonance imaging to guide the management of patients with stable coronary artery disease
- PMID: 22992411
- PMCID: PMC3533866
- DOI: 10.1186/1532-429X-14-65
Design and rationale of the MR-INFORM study: stress perfusion cardiovascular magnetic resonance imaging to guide the management of patients with stable coronary artery disease
Abstract
Background: In patients with stable coronary artery disease (CAD), decisions regarding revascularisation are primarily driven by the severity and extent of coronary luminal stenoses as determined by invasive coronary angiography. More recently, revascularisation decisions based on invasive fractional flow reserve (FFR) have shown improved event free survival. Cardiovascular magnetic resonance (CMR) perfusion imaging has been shown to be non-inferior to nuclear perfusion imaging in a multi-centre setting and superior in a single centre trial. In addition, it is similar to invasively determined FFR and therefore has the potential to become the non-invasive test of choice to determine need for revascularisation.
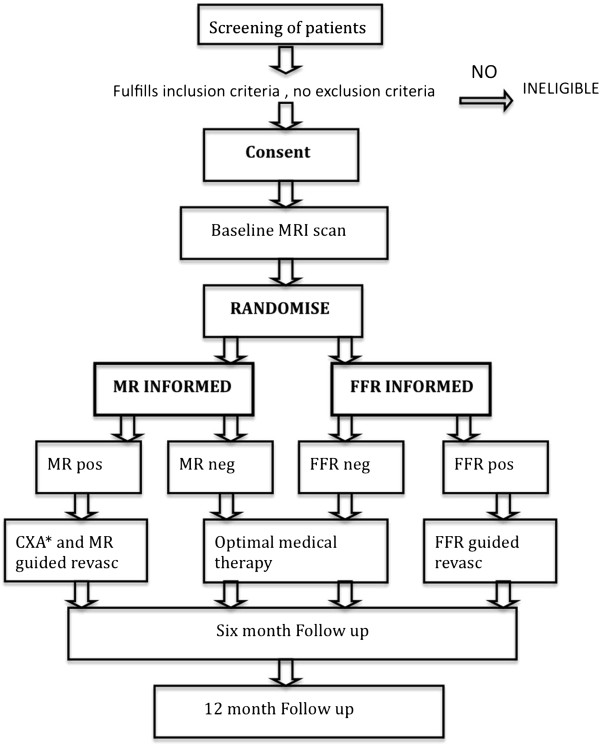
Trial design: The MR-INFORM study is a prospective, multi-centre, randomised controlled non-inferiority, outcome trial. The objective is to compare the efficacy of two investigative strategies for the management of patients with suspected CAD. Patients presenting with stable angina are randomised into two groups: 1) The FFR-INFORMED group has subsequent management decisions guided by coronary angiography and fractional flow reserve measurements. 2) The MR-INFORMED group has decisions guided by stress perfusion CMR. The primary end-point will be the occurrence of major adverse cardiac events (death, myocardial infarction and repeat revascularisation) at one year. Clinical trials.gov identifier NCT01236807.
Conclusion: MR INFORM will assess whether an initial strategy of CMR perfusion is non-inferior to invasive angiography supplemented by FFR measurements to guide the management of patients with stable coronary artery disease. Non-inferiority of CMR perfusion imaging to the current invasive reference standard (FFR) would establish CMR perfusion imaging as an attractive non-invasive alternative to current diagnostic pathways.
Figures
References
-
- Shaw LJ, Berman DS, Maron DJ, Mancini GB, Hayes SW, Hartigan PM, Weintraub WS, O'Rourke RA, Dada M, Spertus JA. et al.Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation. 2008;117:1283–1291. doi: 10.1161/CIRCULATIONAHA.107.743963. - DOI - PubMed
-
- Hachamovitch R, Hayes SW, Friedman JD, Cohen I, Berman DS. Comparison of the short-term survival benefit associated with revascularization compared with medical therapy in patients with no prior coronary artery disease undergoing stress myocardial perfusion single photon emission computed tomography. Circulation. 2003;107:2900–2907. doi: 10.1161/01.CIR.0000072790.23090.41. - DOI - PubMed
-
- Tonino P, De Bruyne B, Pijls N, Siebert U, Ikeno F, Vant Veer M, Klauss V, Manoharan G, Engstrom T, Oldroyd K. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. Book Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. 2009. p. 213. (Editor ed.^eds.), vol. 360. pp. 213. City. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
