

Improving the estimation of influenza-related mortality over a seasonal baseline
- PMID: 22992574
- PMCID: PMC3516362
- DOI: 10.1097/EDE.0b013e31826c2dda
Improving the estimation of influenza-related mortality over a seasonal baseline
Abstract
Background: Existing methods for estimation of mortality attributable to influenza are limited by methodological and data uncertainty. We have used proxies for disease incidence of the three influenza cocirculating subtypes (A/H3N2, A/H1N1, and B) that combine data on influenza-like illness consultations and respiratory specimen testing to estimate influenza-associated mortality in the United States between 1997 and 2007.
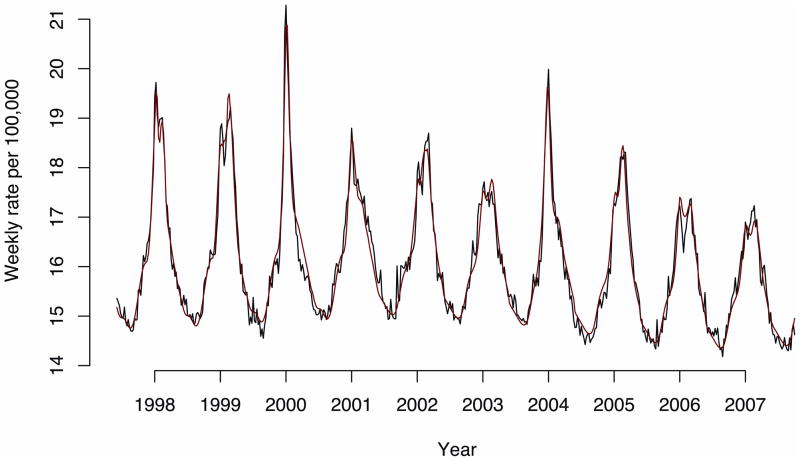
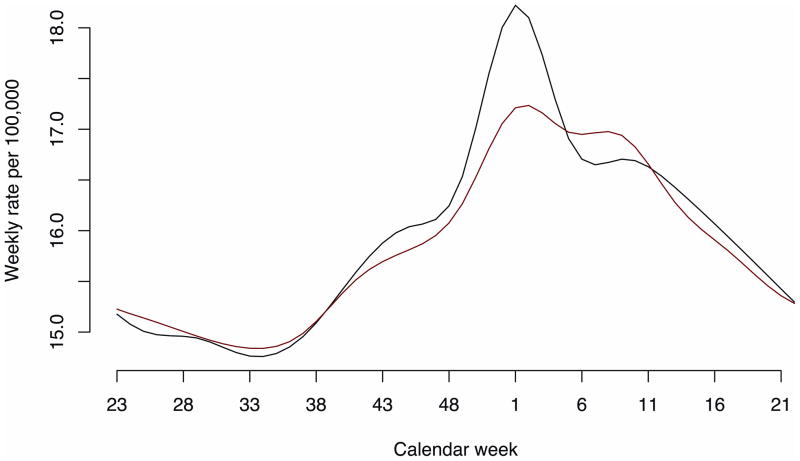
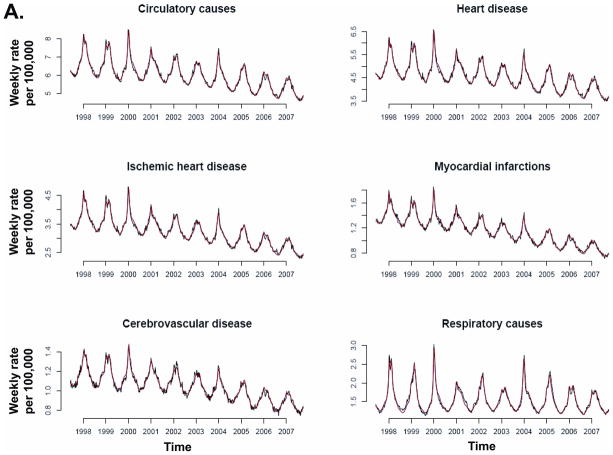
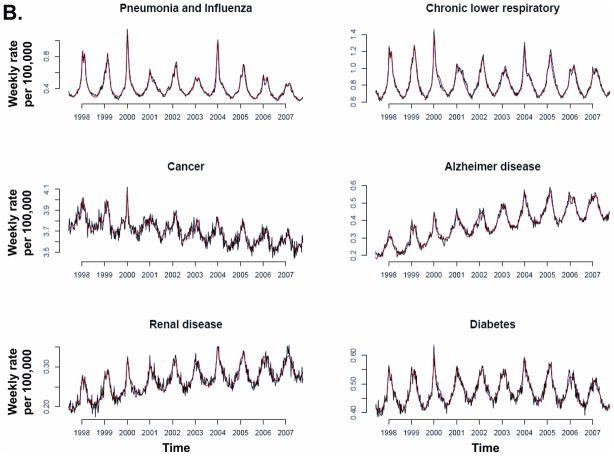
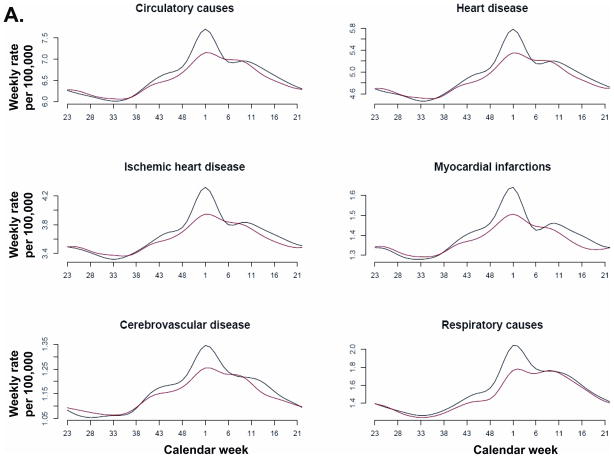
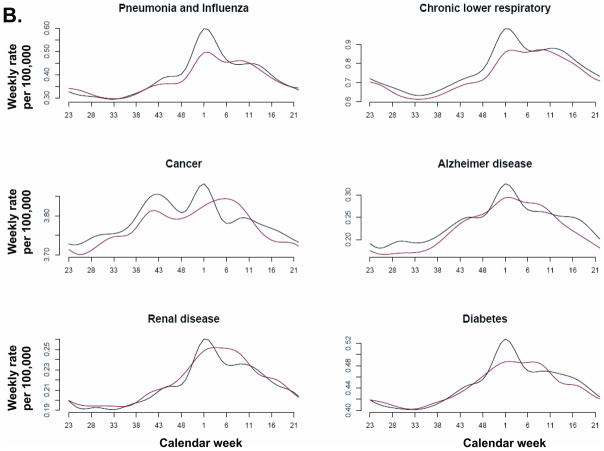
Methods: Weekly mortality rate for several mortality causes potentially affected by influenza was regressed linearly against subtype-specific influenza incidence proxies, adjusting for temporal trend and seasonal baseline, modeled by periodic cubic splines.
Results: Average annual influenza-associated mortality rates per 100,000 individuals were estimated for the following underlying causes of death: for pneumonia and influenza, 1.73 (95% confidence interval = 1.53-1.93); for chronic lower respiratory disease, 1.70 (1.48-1.93); for all respiratory causes, 3.58 (3.04-4.14); for myocardial infarctions, 1.02 (0.85-1.2); for ischemic heart disease, 2.7 (2.23-3.16); for heart disease, 3.82 (3.21-4.4); for cerebrovascular deaths, 0.65 (0.51-0.78); for all circulatory causes, 4.6 (3.79-5.39); for cancer, 0.87 (0.68-1.05); for diabetes, 0.33 (0.26-0.39); for renal disease, 0.19 (0.14-0.24); for Alzheimer disease, 0.41 (0.3-0.52); and for all causes, 11.92 (10.17-13.67). For several underlying causes of death, baseline mortality rates changed after the introduction of the pneumococcal conjugate vaccine.
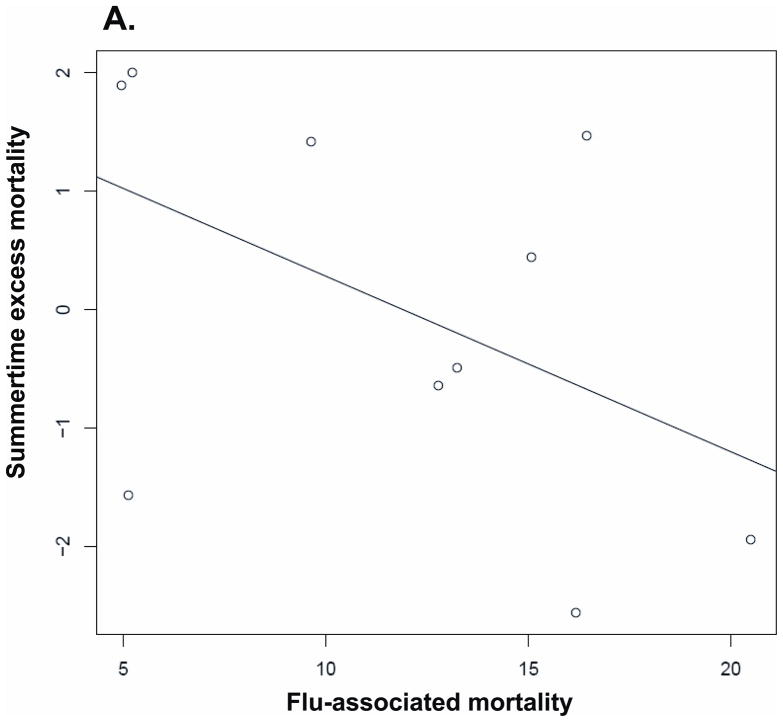
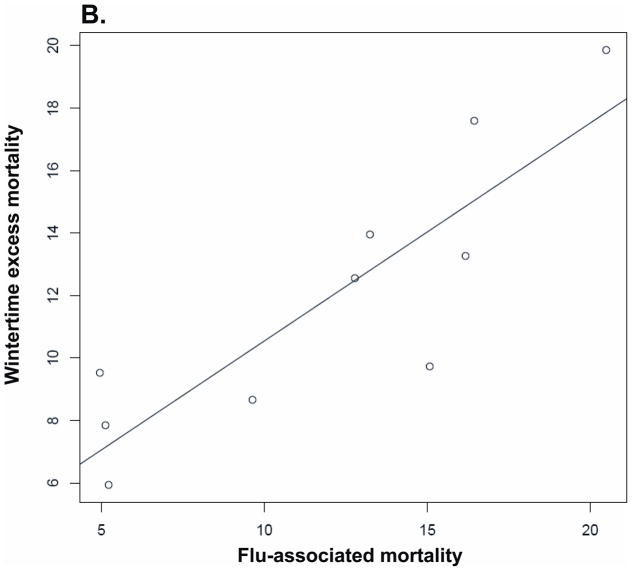
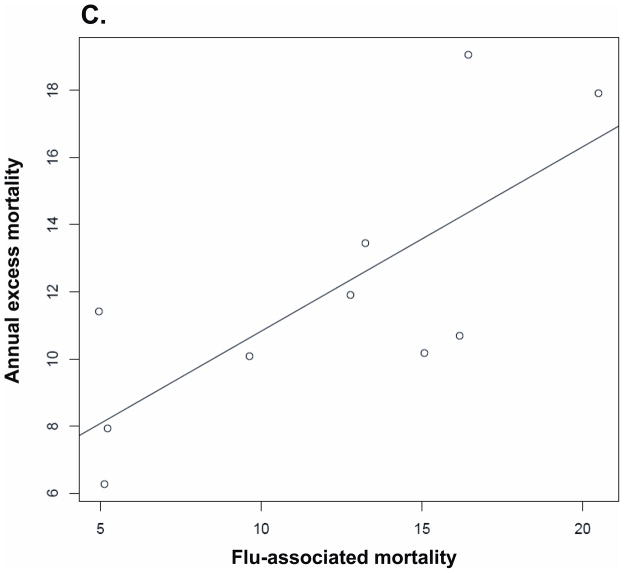
Conclusions: The proposed methodology establishes a linear relation between influenza incidence proxies and excess mortality, rendering temporally consistent model fits, and allowing for the assessment of related epidemiologic phenomena such as changes in mortality baselines.
Conflict of interest statement
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of General Medical Sciences or the National Institutes of Health.
Marc Lipsitch has received consulting fees or honoraria from Pfizer, Novartis, AIR Worldwide, and the Avian/Pandemic Flu Registry (Outcome Sciences and Roche). Other authors declare no conflicts on interest.
Figures
Comment in
-
Time-series analyses of count data to estimate the burden of seasonal infectious diseases.Epidemiology. 2012 Nov;23(6):839-42; discussion 843-4. doi: 10.1097/EDE.0b013e31826cc1df. Epidemiology. 2012. PMID: 23038110 No abstract available.
References
-
- Thompson WW, Shay DK, Weintraub E, et al. Mortality associated with influenza and respiratory syncytial virus in the United States. JAMA. 2003;289:179–186. - PubMed
-
- Dushoff J, Plotkin JB, Viboud C, Earn DJ, Simonsen L. Mortality due to influenza in the United States--an annualized regression approach using multiple-cause mortality data. Am J Epidemiol. 2006;163:181–187. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
