

Diiodothyropropionic acid (DITPA) in the treatment of MCT8 deficiency
- PMID: 22993035
- PMCID: PMC3513545
- DOI: 10.1210/jc.2012-2556
Diiodothyropropionic acid (DITPA) in the treatment of MCT8 deficiency
Abstract
Context: Monocarboxylate transporter 8 (MCT8) is a thyroid hormone-specific cell membrane transporter. MCT8 deficiency causes severe psychomotor retardation and abnormal thyroid tests. The great majority of affected children cannot walk or talk, and all have elevated serum T(3) levels, causing peripheral tissue hypermetabolism and inability to maintain weight. Treatment with thyroid hormone is ineffective. In Mct8-deficient mice, the thyroid hormone analog, diiodothyropropionic acid (DITPA), does not require MCT8 to enter tissues and could be an effective alternative to thyroid hormone treatment in humans.
Objective: The objective of the study was to evaluate the effect and efficacy of DITPA in children with MCT8 deficiency.
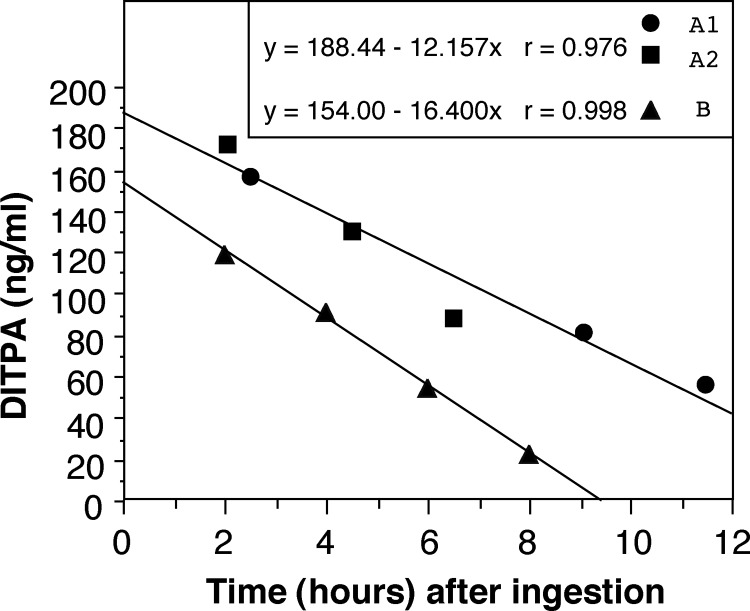
Methods: This was a multicenter report of four affected children given DITPA on compassionate grounds for 26-40 months. Treatment was initiated at ages 8.5-25 months, beginning with a small dose of 1.8 mg, increasing to a maximal 30 mg/d (2.1-2.4 mg/kg · d), given in three divided doses.
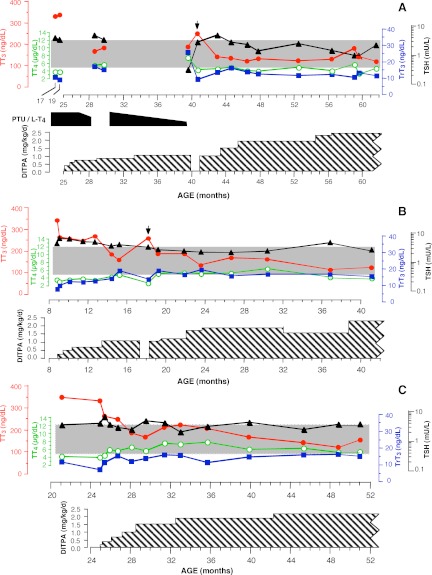
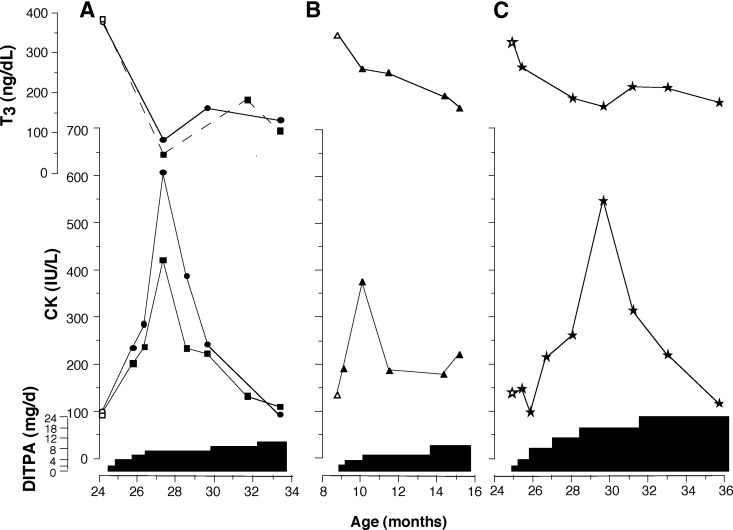
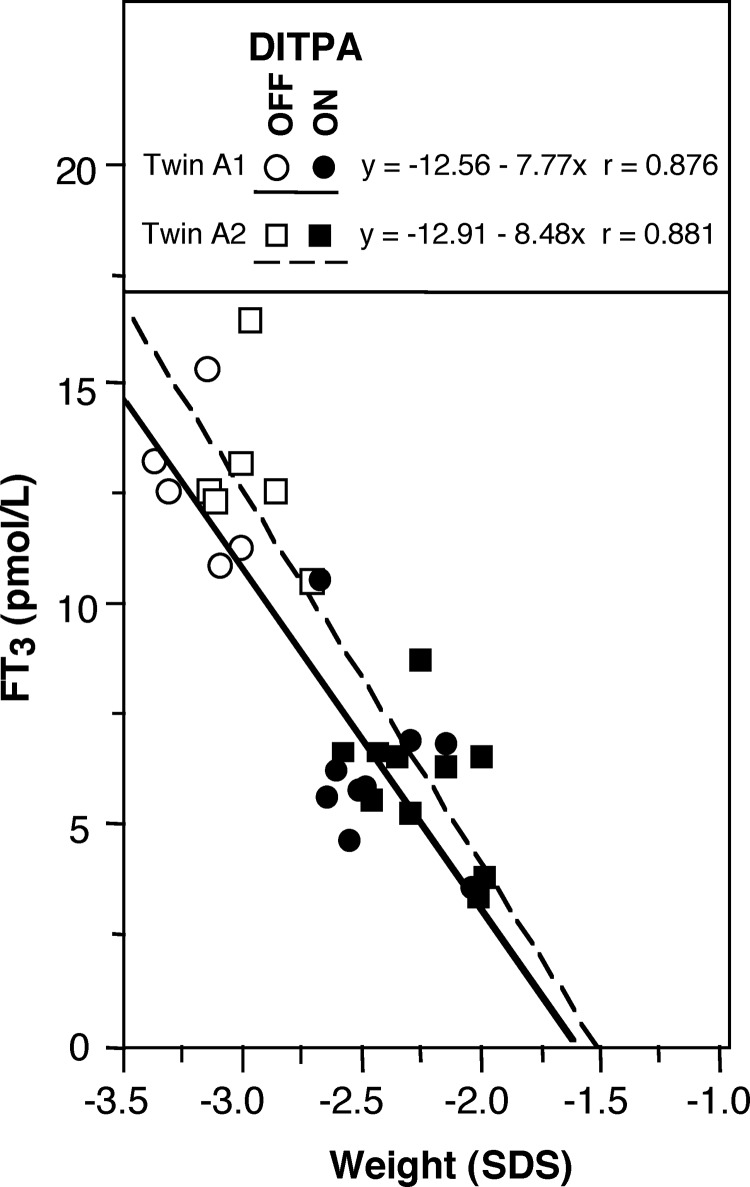
Results: DITPA normalized the elevated serum T(3) and TSH when the dose reached 1 mg/kg · d and T(4) and rT(3) increased to the lower normal range. The following significant changes were also observed: decline in SHBG (in all subjects), heart rate (in three of four), and ferritin (in one of four). Cholesterol increased in two subjects. There was no weight loss and weight gain occurred in two. None of the treated children required a gastric feeding tube or developed seizures. No adverse effects were observed.
Conclusion: DITPA (1-2 mg/kg · d) almost completely normalizes thyroid tests and reduces the hypermetabolism and the tendency for weight loss. The effects of earlier commencement and long-term therapy remain to be determined.
Figures
Comment in
-
Finding the way into the brain without MCT8.J Clin Endocrinol Metab. 2012 Dec;97(12):4362-5. doi: 10.1210/jc.2012-3759. J Clin Endocrinol Metab. 2012. PMID: 23223483 No abstract available.
References
-
- Friesema EC, Grueters A, Biebermann H, Krude H, von Moers A, Reeser M, Barrett TG, Mancilla EE, Svensson J, Kester MH, Kuiper GG, Balkassmi S, Uitterlinden AG, Koehrle J, Rodien P, Halestrap AP, Visser TJ. 2004. Association between mutations in a thyroid hormone transporter and severe X-linked psychomotor retardation. Lancet 364:1435–1437 - PubMed
-
- Friesema EC, Ganguly S, Abdalla A, Manning Fox JE, Halestrap AP, Visser TJ. 2003. Identification of monocarboxylate transporter 8 as a specific thyroid hormone transporter. J Biol Chem 278:40128–40135 - PubMed
-
- Allan W, Herndon CN, Dudley FC. 1944. Some examples of the inheritance of mental deficiency: apparently sex-linked idiocy and microcephaly. Am J Ment Defic 48:325–334
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
