

Loss to programme between HIV diagnosis and initiation of antiretroviral therapy in sub-Saharan Africa: systematic review and meta-analysis
- PMID: 22994151
- PMCID: PMC3895621
- DOI: 10.1111/j.1365-3156.2012.03089.x
Loss to programme between HIV diagnosis and initiation of antiretroviral therapy in sub-Saharan Africa: systematic review and meta-analysis
Abstract
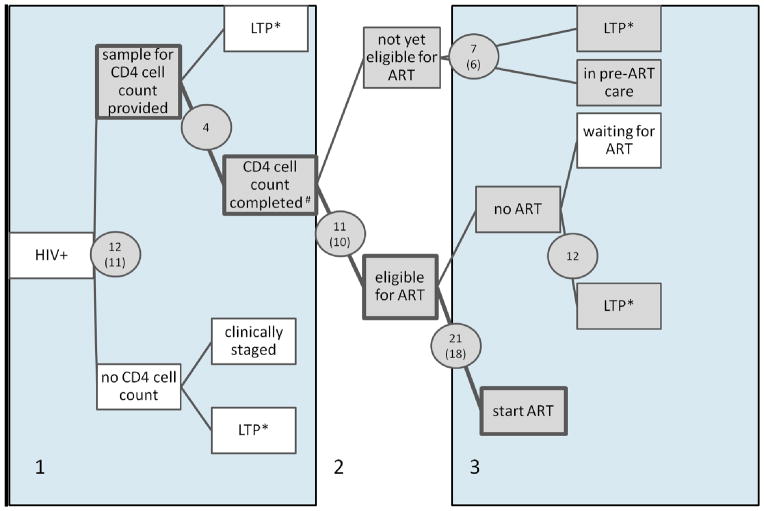
Objectives: To assess the proportion of patients lost to programme (died, lost to follow-up, transferred out) between HIV diagnosis and start of antiretroviral therapy (ART) in sub-Saharan Africa, and determine factors associated with loss to programme.
Methods: Systematic review and meta-analysis. We searched PubMed and EMBASE databases for studies in adults. Outcomes were the percentage of patients dying before starting ART, the percentage lost to follow-up, the percentage with a CD4 cell count, the distribution of first CD4 counts and the percentage of eligible patients starting ART. Data were combined using random-effects meta-analysis.
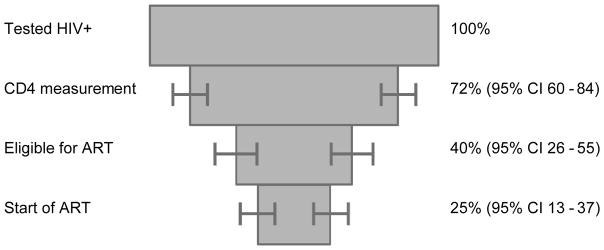
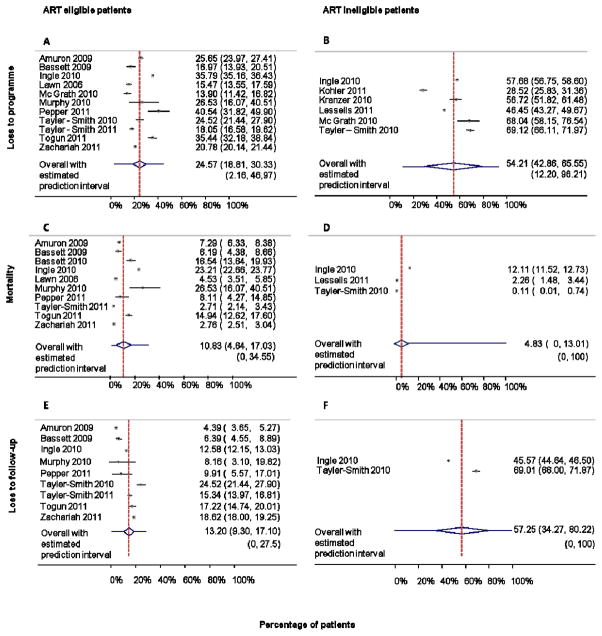
Results: Twenty-nine studies from sub-Saharan Africa including 148,912 patients were analysed. Six studies covered the whole period from HIV diagnosis to ART start. Meta-analysis of these studies showed that of the 100 patients with a positive HIV test, 72 (95% CI 60-84) had a CD4 cell count measured, 40 (95% CI 26-55) were eligible for ART and 25 (95% CI 13-37) started ART. There was substantial heterogeneity between studies (P < 0.0001). Median CD4 cell count at presentation ranged from 154 to 274 cells/μl. Patients eligible for ART were less likely to become lost to programme (25%vs. 54%, P < 0.0001), but eligible patients were more likely to die (11%vs. 5%, P < 0.0001) than ineligible patients. Loss to programme was higher in men, in patients with low CD4 cell counts and low socio-economic status and in recent time periods.
Conclusions: Monitoring and care in the pre-ART time period need improvement, with greater emphasis on patients not yet eligible for ART.
Keywords: Afrique subsaharienne; liens avec les soins; linkage to care; loss to follow‐up; mortalidad; mortality; mortalité; nexo con atención médica; perte au suivi; pre‐ART; pre‐TAR; pré‐ART; pérdida durante el seguimiento; sub‐Saharan Africa; África subsahariana.
© 2012 Blackwell Publishing Ltd.
Figures
References
-
- Braitstein P, Brinkhof MW, Dabis F, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. The Lancet. 2006;367:817–824. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
