

The immunophenotype of T-lymphoblastic lymphoma in children and adolescents: a Children's Oncology Group report
- PMID: 22994934
- PMCID: PMC4008319
- DOI: 10.1111/bjh.12042
The immunophenotype of T-lymphoblastic lymphoma in children and adolescents: a Children's Oncology Group report
Abstract
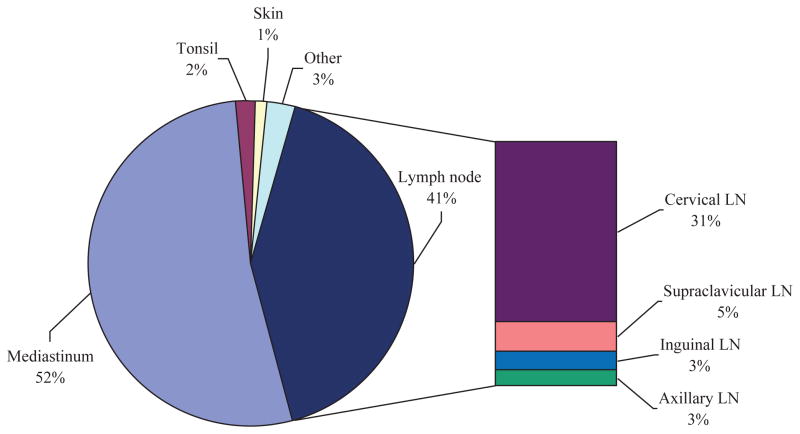
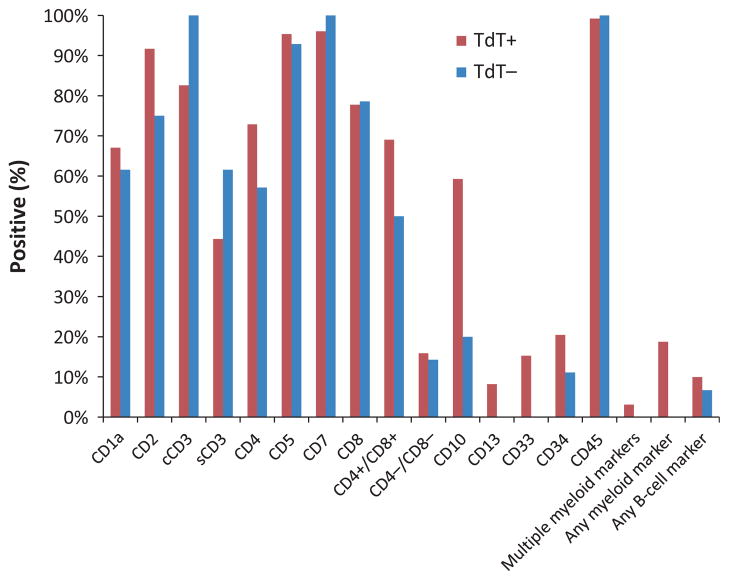
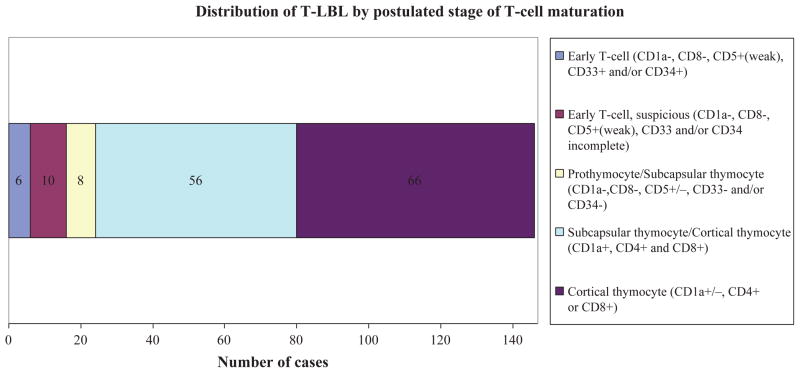
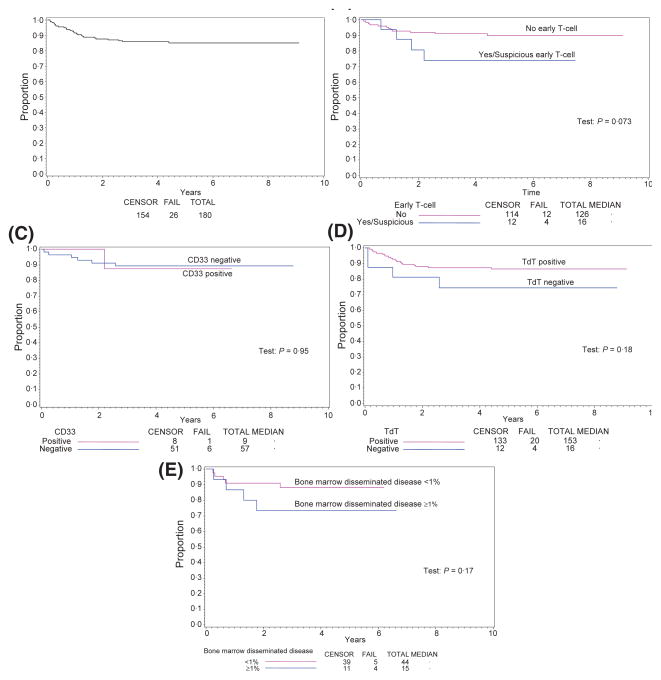
T-lymphoblastic leukaemia (T-ALL) and T-lymphoblastic lymphoma (T-LBL) are neoplasms derived from immature lymphoid cells of T-cell lineage. These neoplasms are biologically similar, but significant differences may exist between the two given their clinical differences. Although ample data regarding the immunophenotypic characterization T-ALL are available, there is a paucity of such data in children and adolescents with T-LBL. We used flow cytometry and/or immunohistochemistry to characterize the immunophenotypic profile of 180 children and adolescents with newly diagnosed T-LBL enrolled in the Children's Oncology Group 5971 study. Multiple T-cell, B-cell, myeloid, and other markers were evaluated. We identified diagnostically useful immunophenotypic features of T-LBL as well as distinct immunophenotypic subgroups, although none of these was statistically related to event-free or overall survival in this retrospective analysis. Further studies of biologically and immunophenotypically distinct subgroups of T-LBL, such as the early T-cell precursor phenotype, are warranted.
© 2012 Blackwell Publishing Ltd.
Figures
References
-
- Abromowitch M, Sposto R, Perkins S, Zwick D, Siegel S, Finlay J, Cairo MS. Shortened intensified multi-agent chemotherapy and non-cross resistant maintenance therapy for advanced lymphoblastic lymphoma in children and adolescents: report from the Children’s Oncology Group. British Journal of Haematology. 2008;143:261–267. - PMC - PubMed
-
- Al Khabori M, Samiee S, Fung S, Xu W, Brandwein J, Patterson B, Brien W, Chang H. Adult precursor T-lymphoblastic leukemia/lymphoma with myeloid-associated antigen expression is associated with a lower complete remission rate following induction chemotherapy. Acta Haematologica. 2008;120:5–10. - PubMed
-
- Bell JJ, Bhandoola A. The earliest thymic progenitors for T cells possess myeloid line-age potential. Nature. 2008;452:764–767. - PubMed
-
- Bene MC, Castoldi G, Knapp W, Ludwig WD, Matutes E, Orfao A, Van’t Veer MB. Proposals for the immunological classification of acute leukemias. European Group for the Immunological Characterization of Leukemias (EGIL) Leukemia. 1995;9:1783–1786. - PubMed
-
- Burkhardt B. Paediatric lymphoblastic T-cell leukaemia and lymphoma: one or two diseases? British Journal of Haematology. 2009;149:653–668. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
