

Evaluating swallowing muscles essential for hyolaryngeal elevation by using muscle functional magnetic resonance imaging
- PMID: 22995662
- PMCID: PMC3563921
- DOI: 10.1016/j.ijrobp.2012.07.2370
Evaluating swallowing muscles essential for hyolaryngeal elevation by using muscle functional magnetic resonance imaging
Abstract
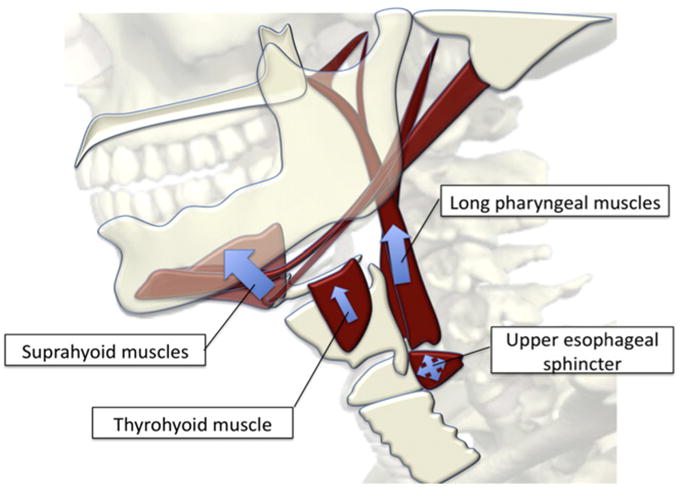
Purpose: Reduced hyolaryngeal elevation, a critical event in swallowing, is associated with radiation therapy. Two muscle groups that suspend the hyoid, larynx, and pharynx have been proposed to elevate the hyolaryngeal complex: the suprahyoid and longitudinal pharyngeal muscles. Thought to assist both groups is the thyrohyoid, a muscle intrinsic to the hyolaryngeal complex. Intensity modulated radiation therapy guidelines designed to preserve structures important to swallowing currently exclude the suprahyoid and thyrohyoid muscles. This study used muscle functional magnetic resonance imaging (mfMRI) in normal healthy adults to determine whether both muscle groups are active in swallowing and to test therapeutic exercises thought to be specific to hyolaryngeal elevation.
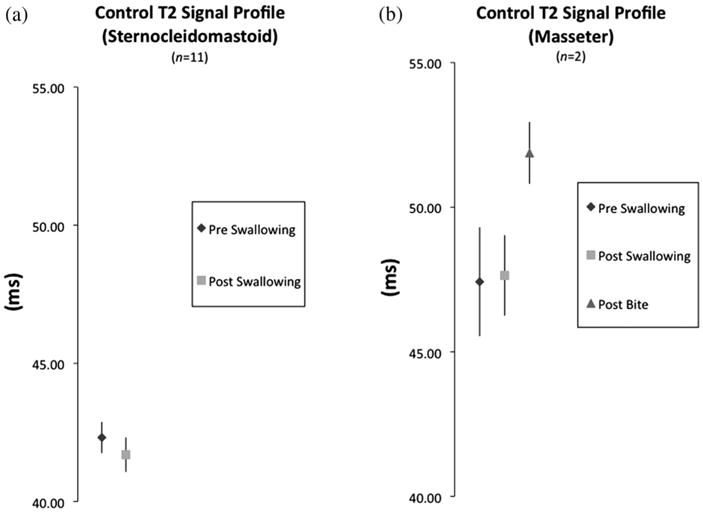
Methods and materials: mfMRI data were acquired from 11 healthy subjects before and after normal swallowing and after swallowing exercise regimens (the Mendelsohn maneuver and effortful pitch glide). Whole-muscle transverse relaxation time (T2 signal, measured in milliseconds) profiles of 7 test muscles were used to evaluate the physiologic response of each muscle to each condition. Changes in effect size (using the Cohen d measure) of whole-muscle T2 profiles were used to determine which muscles underlie swallowing and swallowing exercises.
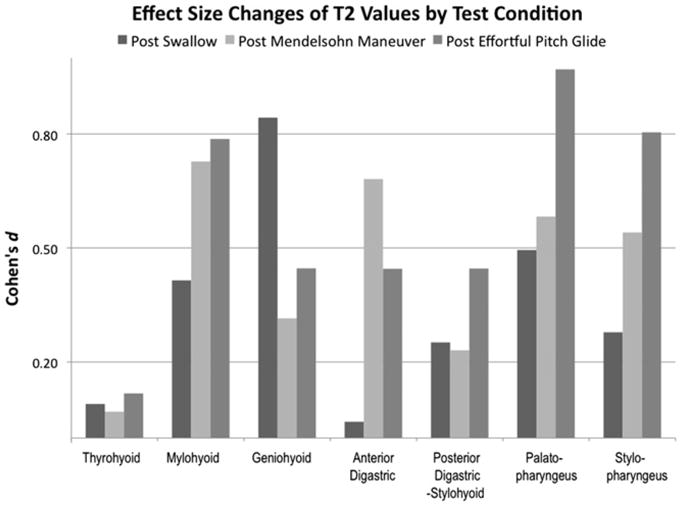
Results: Post-swallowing effect size changes (where a d value of >0.20 indicates significant activity during swallowing) for the T2 signal profile of the thyrohyoid was a d value of 0.09; a d value of 0.40 for the mylohyoid, 0.80 for the geniohyoid, 0.04 for the anterior digastric, and 0.25 for the posterior digastric-stylohyoid in the suprahyoid muscle group; and d values of 0.47 for the palatopharyngeus and 0.28 for the stylopharyngeus muscles in the longitudinal pharyngeal muscle group. The Mendelsohn maneuver and effortful pitch glide swallowing exercises showed significant effect size changes for all muscles tested, except for the thyrohyoid.
Conclusions: Muscles of both the suprahyoid and the longitudinal pharyngeal muscle groups are active in swallowing, and both swallowing exercises effectively target muscles elevating the hyolaryngeal complex. mfMRI is useful in testing swallowing muscle function.
Copyright © 2013 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: none.
Figures
Comment in
-
Function, muscles, and sparing by IMRT for head-and-neck cancer.Int J Radiat Oncol Biol Phys. 2013 Mar 1;85(3):577-8. doi: 10.1016/j.ijrobp.2012.08.040. Int J Radiat Oncol Biol Phys. 2013. PMID: 23374990 No abstract available.
References
-
- Rosenthal DI, Lewin JS, Eisbruch A. Prevention and treatment of dysphagia and aspiration after chemoradiation for head and neck cancer. J Clin Oncol. 2006;24:2636. - PubMed
-
- Pauloski BR, Rademaker AW, Logemann JA, et al. Relationship between swallow motility disorders on videofluorography and oral intake in patients treated for head and neck cancer with radiotherapy with or without chemotherapy. Head Neck. 2006;28:1069–1076. - PubMed
-
- Eisbruch A, Schwartz M, Rasch C, et al. Dysphagia and aspiration after chemoradiotherapy for head-and-neck cancer: which anatomic structures are affected and can they be spared by IMRT? Int J Radiat Oncol Biol Phys. 2004;60:1425–1439. - PubMed
-
- Levendag PC, Teguh DN, Voet P, et al. Dysphagia disorders in patients with cancer of the oropharynx are significantly affected by the radiation therapy dose to the superior and middle constrictor muscle: a dose-effect relationship. Radiother Oncol. 2007;85:64–73. - PubMed
-
- Caglar HB, Tishler RB, Othus M, et al. Dose to larynx predicts for swallowing complications after intensity-modulated radiotherapy. Int J Radiat Oncol Biol Phys. 2008;72:1110–1118. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
