

HIV infection and stroke: current perspectives and future directions
- PMID: 22995692
- PMCID: PMC3460367
- DOI: 10.1016/S1474-4422(12)70205-3
HIV infection and stroke: current perspectives and future directions
Abstract
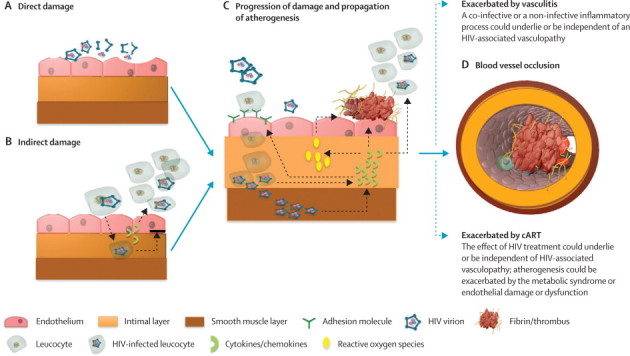
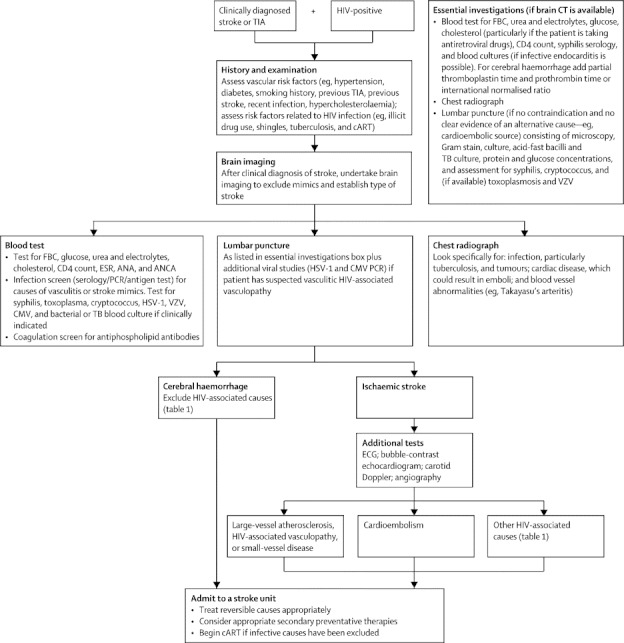
HIV infection can result in stroke via several mechanisms, including opportunistic infection, vasculopathy, cardioembolism, and coagulopathy. However, the occurrence of stroke and HIV infection might often be coincidental. HIV-associated vasculopathy describes various cerebrovascular changes, including stenosis and aneurysm formation, vasculitis, and accelerated atherosclerosis, and might be caused directly or indirectly by HIV infection, although the mechanisms are controversial. HIV and associated infections contribute to chronic inflammation. Combination antiretroviral therapies (cART) are clearly beneficial, but can be atherogenic and could increase stroke risk. cART can prolong life, increasing the size of the ageing population at risk of stroke. Stroke management and prevention should include identification and treatment of the specific cause of stroke and stroke risk factors, and judicious adjustment of the cART regimen. Epidemiological, clinical, biological, and autopsy studies of risk, the pathogenesis of HIV-associated vasculopathy (particularly of arterial endothelial damage), the long-term effects of cART, and ideal stroke treatment in patients with HIV are needed, as are antiretrovirals that are without vascular risk.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures
References
-
- Feigin VL, Lawes CMM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. 2009;8:355–369. - PubMed
-
- Feigin VL. Stroke in developing countries: can the epidemic be stopped and outcomes improved? Lancet Neurol. 2007;6:94–97. - PubMed
-
- Walker R, Whiting D, Unwin N. Stroke incidence in rural and urban Tanzania: a prospective, community-based study. Lancet Neurol. 2010;9:786–792. - PubMed
-
- Emsley HCA, Hopkins SJ. Acute ischaemic stroke and infection: recent and emerging concepts. Lancet Neurol. 2008;7:341–353. - PubMed
-
- Quinn TC. Global burden of the HIV pandemic. Lancet. 1996;348:99–106. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
