

Botulinum neurotoxin type A for the treatment of benign prostatic hyperplasia: randomized study comparing two doses
- PMID: 22997495
- PMCID: PMC3446647
- DOI: 10.1100/2012/463574
Botulinum neurotoxin type A for the treatment of benign prostatic hyperplasia: randomized study comparing two doses
Abstract
Purpose: To assess the efficacy and safety of intraprostatic injection of two botulinum neurotoxin type A (BoNT-A) doses for the treatment of benign prostatic hyperplasia (BPH).
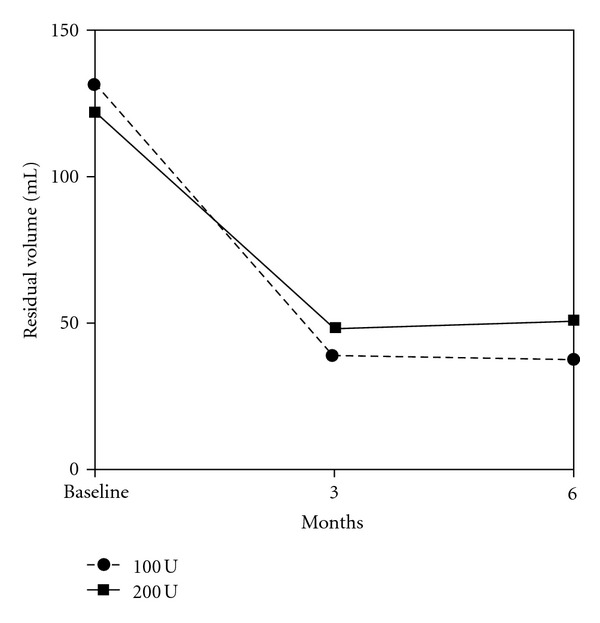
Materials and methods: Men with symptomatic BPH who failed medical treatment were randomized to receive 100 U or 200 U of BoNT-A into the prostate. The International Prostatic Symptom Score (IPSS), maximum flow rate (Q(max)), post-void residual volume (PVR), PSA levels and prostate volume before injection and after 3 and 6 months were evaluated. Adverse events were compared between the groups.
Results: Thirty four patients were evaluated, including 17 in the BoNT-A 100 U group and 17 in the BoNT-A 200 U group. Baseline characteristics were similar in both groups. Both doses produced significant improvements in IPSS, Q(max) and PVR after 3 and 6 months and both doses promoted comparable effects. Prostate volume was affected by 200 U BoNT-A injection only after 6 months of treatment. PSA levels were significantly affected in the 100 U group only after 6 months of treatment. In the 200 U group, PSA levels were significantly decreased after 3 and 6 months. The complication rate was similar in both groups.
Conclusions: Efficacy and safety of both BoNT-A doses are similar for BPH treatment in the short term followup.
Figures


Similar articles
-
Intraprostatic botulinum neurotoxin type a injection for benign prostatic hyperplasia: preliminary results with a newly purified neurotoxin.Acta Med Okayama. 2012;66(4):291-7. doi: 10.18926/AMO/48668. Acta Med Okayama. 2012. PMID: 22918201 Clinical Trial.
-
Therapeutic effects of add-on botulinum toxin A on patients with large benign prostatic hyperplasia and unsatisfactory response to combined medical therapy.Scand J Urol Nephrol. 2009;43(3):206-11. doi: 10.1080/00365590902811537. Scand J Urol Nephrol. 2009. PMID: 19308807 Clinical Trial.
-
Outcome of Botulinum Toxin-A intraprostatic injection for benign prostatic hyperplasia induced lower urinary tract symptoms: A prospective multicenter study.Prostate. 2019 Aug;79(11):1221-1225. doi: 10.1002/pros.23805. Epub 2019 Jun 12. Prostate. 2019. PMID: 31189024
-
Intraprostatic Botulinum Neurotoxin Type A Injection for Benign Prostatic Hyperplasia-A Spotlight in Reality.Toxins (Basel). 2016 Apr 26;8(5):126. doi: 10.3390/toxins8050126. Toxins (Basel). 2016. PMID: 27128942 Free PMC article. Review.
-
Botulinum neurotoxin A for male lower urinary tract symptoms.Curr Opin Urol. 2011 Jan;21(1):13-21. doi: 10.1097/MOU.0b013e3283410117. Curr Opin Urol. 2011. PMID: 21099691 Review.
Cited by
-
Transperineal intraprostatic injection of botulinum neurotoxin A vs transurethral resection of prostate for management of lower urinary tract symptoms secondary to benign prostate hyperplasia: A prospective randomised study.Arab J Urol. 2019 Oct 3;17(4):270-278. doi: 10.1080/2090598X.2019.1662214. eCollection 2019. Arab J Urol. 2019. PMID: 31723444 Free PMC article.
-
Lysozyme gene treatment in testosterone induced benign prostate hyperplasia rat model and comparasion of its' effectiveness with botulinum toxin injection.Int Braz J Urol. 2017 Nov-Dec;43(6):1167-1175. doi: 10.1590/S1677-5538.IBJU.2016.0677. Int Braz J Urol. 2017. PMID: 28727388 Free PMC article.
-
New medical treatments for lower urinary tract symptoms due to benign prostatic hyperplasia and future perspectives.BMC Urol. 2016 Sep 15;16(1):58. doi: 10.1186/s12894-016-0176-0. BMC Urol. 2016. PMID: 27629059 Free PMC article. Review.
-
Clinical Application of Botulinum Neurotoxin in Lower-Urinary-Tract Diseases and Dysfunctions: Where Are We Now and What More Can We Do?Toxins (Basel). 2022 Jul 18;14(7):498. doi: 10.3390/toxins14070498. Toxins (Basel). 2022. PMID: 35878235 Free PMC article. Review.
-
Botulinum toxin-what urologic uses does the data support?Curr Urol Rep. 2013 Jun;14(3):227-34. doi: 10.1007/s11934-013-0326-9. Curr Urol Rep. 2013. PMID: 23625366 Review.
References
-
- Clifford GM, Farmer RDT. Medical therapy for benign prostatic hyperplasia: a review of the literature. European Urology. 2000;38(1):2–19. - PubMed
-
- Oesterling JE. Benign prostatic hyperplasia—medical and minimally invasive treatment options. The New England Journal of Medicine. 1995;332(2):99–109. - PubMed
-
- de La Rosette JJMCH, Alivizatos G, Madersbacher S, et al. EAU guidelines on Benign Prostatic Hyperplasia (BPH) European Urology. 2001;40(3):256–264. - PubMed
-
- Lepor H, Williford WO, Barry MJ, et al. The efficacy of terazosin, finasteride, or both in benign prostatic hyperplasia. The New England Journal of Medicine. 1996;335(8):533–539. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
