

Comparative cost-effectiveness of interventions to improve medication adherence after myocardial infarction
- PMID: 22998129
- PMCID: PMC3523366
- DOI: 10.1111/j.1475-6773.2012.01462.x
Comparative cost-effectiveness of interventions to improve medication adherence after myocardial infarction
Abstract
Objective: To evaluate the comparative cost-effectiveness of interventions to improve adherence to evidence-based medications among postmyocardial infarction (MI) patients.
Data sources/study setting: Cost-effectiveness analysis.
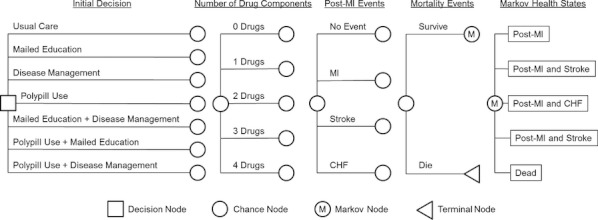
Study design: We developed a Markov model simulating a hypothetical cohort of 65-year-old post-MI patients who were prescribed secondary prevention medications. We evaluated mailed education, disease management, polypill use, and combinations of these interventions. The analysis was performed from a societal perspective over a lifetime horizon. The main outcome was an incremental cost-effectiveness ratio (ICER) as measured by cost per quality-adjusted life year (QALY) gained.
Data collection/extraction methods: Model inputs were extracted from published literature.
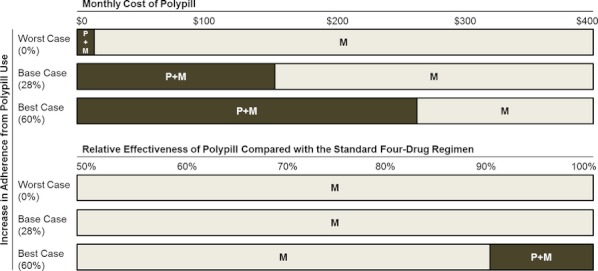
Principal findings: Compared with usual care, only mailed education had both improved health outcomes and reduced spending. Mailed education plus disease management, disease management, polypill use, polypill use plus mailed education, and polypill use plus disease management cost were $74,600, $69,200, $133,000, $113,000, and $142,900 per QALY gained, respectively. In an incremental analysis, only mailed education had an ICER of less than $100,000 per QALY and was therefore the optimal strategy. Polypill use, particularly when combined with mailed education, could be cost effective, and potentially cost saving if its price decreased to less than $100 per month.
Conclusions: Mailed education and a polypill, once available, may be the cost-saving strategies for improving post-MI medication adherence.
© Health Research and Educational Trust.
Figures

References
-
- Agency for Healthcare Research and Quality. 2011. “Closing the Quality Gap Series: Comparative Effectiveness of Medication Adherence Interventions” [accessed on March 31, 2012]. Available at http://www.effectivehealthcare.ahrq.gov/ehc/products/296/764/Medication-.... - PubMed
-
- Arias E. 2010. “United States Life Tables, 2006. National Vital Statistics Report. Volume 58, Number 21. Hyattsville, MD. National Center for Health Statistics; 2010” [accessed March 31, 2012]. Available at http://www.cdc.gov/nchs/data/nvsr/nvsr58/nvsr58_21.pdf.
-
- Bangalore S, Kamalakkannan G, Parker S, Messerli FH. “Fixed-Dose Combinations Improve Medication Compliance: A Meta-Analysis”. American Journal of Medicine. 2007;120(8):713–9. - PubMed
-
- Benner JS, Glynn RJ, Mogun H, Weinstein MC, Avorn J. “Long-Term Persistence in Use of Statin Therapy in Elderly Patients”. Journal of the American Medical Association. 2002;288(4):455–61. - PubMed
-
- Brønnum-Hansen H, Jørgensen T, Davidsen M, Madsen M, Osler M, Gerdes LU, Schroll M. “Survival and Cause of Death after Myocardial Infarction: The Danish MONICA Study”. Journal of Clinical Epidemiology. 2001;54(12):1244–50. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
