

Endovascular coiling versus neurosurgical clipping in patients with unruptured intracranial aneurysm: a systematic review
- PMID: 22998483
- PMCID: PMC3519507
- DOI: 10.1186/1471-2377-12-99
Endovascular coiling versus neurosurgical clipping in patients with unruptured intracranial aneurysm: a systematic review
Abstract
Background: To compare the effects of endovascular coiling and neurosurgical clipping in patients with unruptured intracranial aneurysm.
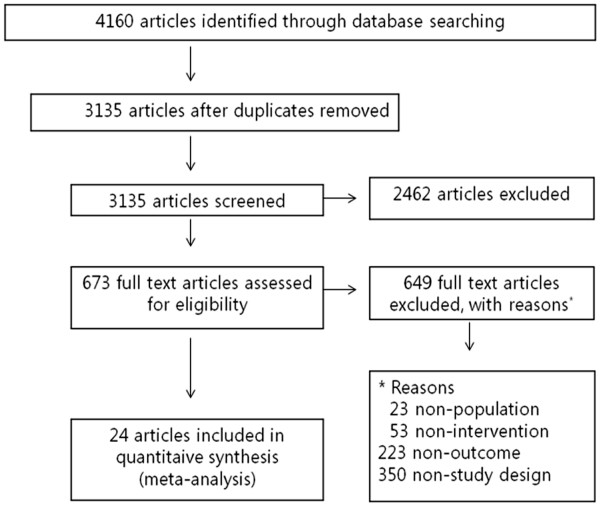
Methods: Sixteen electronic databases were searched for articles published between 1950 and July 2010 to compare clinical outcomes of clipping and coiling. Researchers reviewed all searched articles and extracted data independently. The quality of studies and evidence were evaluated using MINORS and GRADEprofiler, respectively. The odds ratio (OR) was calculated using the inverse variance meta-analysis method for each study outcome. To assess heterogeneity of ORs across cohorts, Cochran's Q statistic and I² were used.
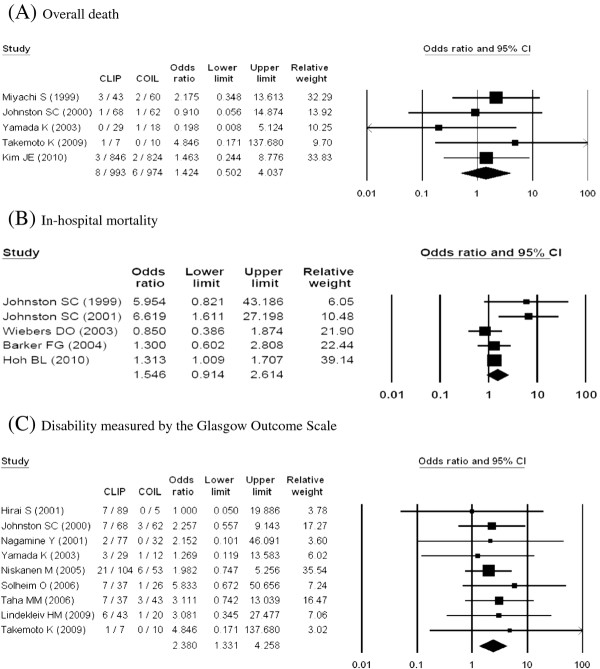
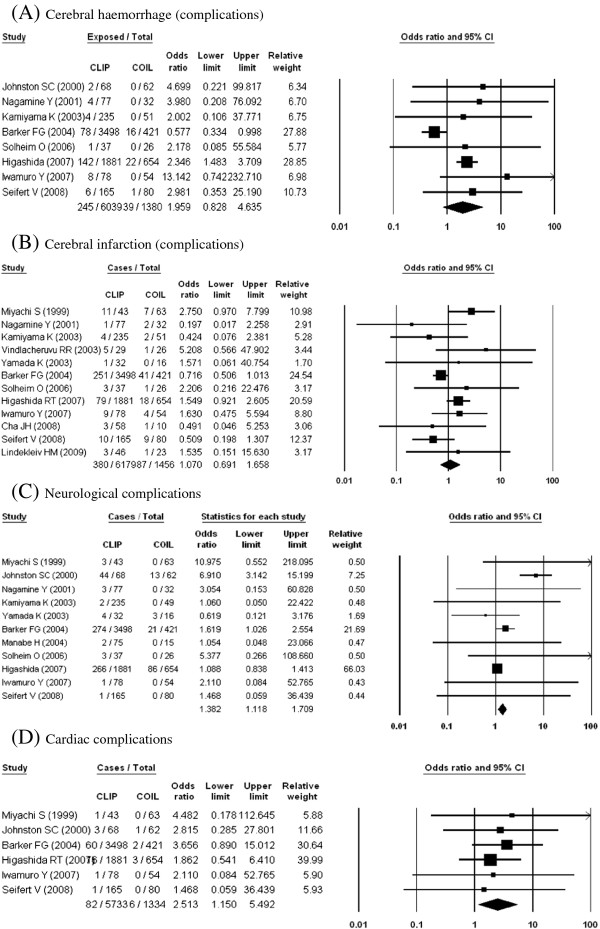
Results: Of 4160 studies, 24 were identified (n = 31865). Clipping resulted in significantly higher disability using the Glasgow Outcome Scale (OR, 2.38; 95% CI, 1.33-4.26) and Modified Rankin Scale (OR, 2.83; 95% CI, 1.42-5.63) when compared with coiling. ORs for complications were also higher with clipping (ORs for neurological and cardiac complications were 1.94 with a 95% confidence interval [CI] of 1.09-3.47 and 2.51 with a 95% CI of 1.15-5.50). Clipping resulted in significantly greater disability in the short term (≤6 m)(OR on the Glasgow Outcome Scale, 2.72; 95% CI, 1.16-6.34), but not in the long term (>6 m)(OR for Glasgow Outcome Scale, 2.12; 95% CI, 0.93-4.84).
Conclusions: Coiling was a better procedure for treatment of unruptured intracranial aneurysm in terms of disability, complications, especially in the short term. Because of the limitations of the reviewed studies, further studies are required to support the present results.
Figures
References
-
- Byun HS. Recent trends in the treatment of cerebral aneurysms: comparison between endovascular coil embolization and surgical clipping. Neurointervention. 2009;4:1–5.
-
- Yoshimoto Y, Wakai S. Cost-effectiveness analysis of screening for asymptomatic, unruptured intracranial aneurysms. A mathematical model. Stroke. 1999;30(8):1621–1627. - PubMed
-
- Van Der Schaaf I, Algra A, Wermer M, Molyneux A, Clarke M, Van Gijn J, Rinkel G. Endovascular coiling versus neurosurgical clipping for patients with aneurysmal subarachnoid haemorrhage. Cochrane Database Syst Rev. 2005;19(4):CD003085. - PubMed
-
- Komotar RJ, Mocco J, Solomon RA. Guidelines for the surgical treatment of unruptured intracranial aneurysms: the first annual J. Lawrence pool memorial research symposium--controversies in the management of cerebral aneurysms. Neurosurgery. 2008;62(1):183–193. doi: 10.1227/01.NEU.0000311076.64109.2E. discussion 193–184. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
