

Evidence of lifestyle modification in the management of hypercholesterolemia
- PMID: 22998604
- PMCID: PMC3584303
- DOI: 10.2174/157340313805076313
Evidence of lifestyle modification in the management of hypercholesterolemia
Abstract
Background: Coronary heart disease (CHD) is the leading cause of morbidity and mortality worldwide. The growth of ageing populations in developing countries with progressively urbanized lifestyles are major contributors. The key risk factors for CHD such as hypercholesterolemia, diabetes mellitus, and obesity are likely to increase in the future. These risk factors are modifiable through lifestyle.
Objectives: To review current literature on the potential benefit of cholesterol lowering in CHD risk reduction with a particular focus on the evidence of non-pharmacological/lifestyle management of hypercholesterolemia.
Methods: Medline/PubMed systematic search was conducted using a two-tier approach limited to all recent English language papers. Primary search was conducted using key words and phrases and all abstracts were subsequently screened and relevant papers were selected. The next tier of searching was conducted by (1) reviewing the citation lists of the selected papers and (2) by using PubMed weblink for related papers. Over 3600 reports were reviewed.
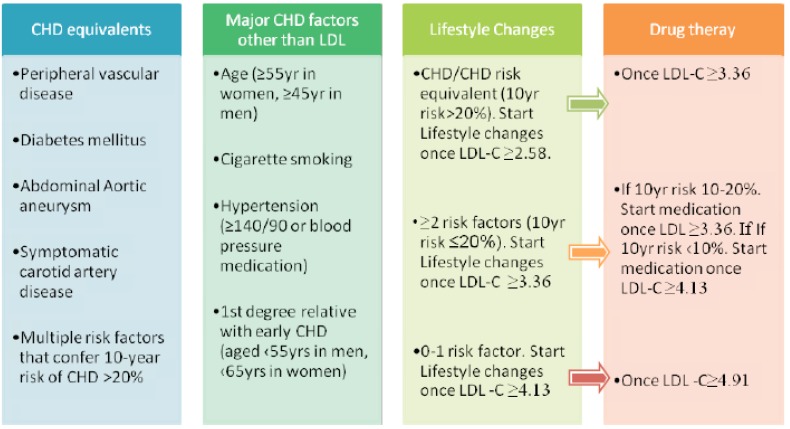
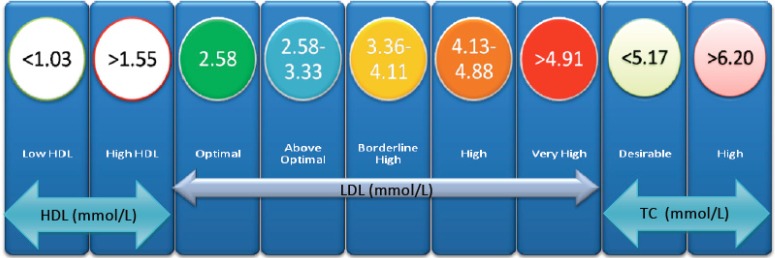
Results: Target cholesterol levels set out in various guidelines could be achieved by lifestyle changes, including diet, weight reduction, and increased physical activity with the goal of reducing total cholesterol to <200 mg/dL and LDL-C<100 mg/dL. Various dietary constituents such as green tea, plant sterols, soy protein have important influences on total cholesterol. Medical intervention should be reserved for those patients who have not reached this goal after 3 months of non-pharmacological approach.
Conclusion: CHD remains as a leading cause of death worldwide and hypercholesterolemia is an important cause of CHD. Non-pharmacological methods provide initial as well as long-term measures to address this issue.
Figures
References
-
- Gibler Wb, Cannon Cp, Blomkalns Al, et al. Practical implementation of the guidelines for unstable angina/non-ST-segment elevation myocardial infarction in the emergency department: a scientific statement from the American Heart Association Council on Clinical Cardiology (Subcommittee on Acute Cardiac Care), Council on Cardiovascular Nursing, and Quality of Care and Outcomes Research Interdisciplinary Working Group, in Collaboration With the Society of Chest Pain Centers. Circulation. 2005;111(20 ):2699–2710. - PubMed
-
- Lloyd-Jones Dm, Larson Mg, Beiser A, Levy D. Lifetime risk of developing coronary heart disease. Lancet. 1999;353(9147 ):89–92. - PubMed
-
- Duvall Wl, Vorchheimer Da. Multi-bed vascular disease and atherothrombosis scope of the problem. J Thromb Thrombolysis. 2004;17(1 ):51–61. - PubMed
-
- Yusuf S, John Cairns J, Camm J, Fallen El, Gersh Bj. Evidence-Based Cardiology. John Wiley & Sons Incorporated. 2003:3–15.
-
- Verschuren Wm, Jacobs Dr, Bloemberg Bp, et al. Serum total cholesterol and long-term coronary heart disease mortality in different cultures. Twenty-five-year follow-up of the seven countries study. JAMA. 1995;274(2 ):131–136. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
