

Quantification of absolute myocardial perfusion in patients with coronary artery disease: comparison between cardiovascular magnetic resonance and positron emission tomography
- PMID: 22999722
- PMCID: PMC7611225
- DOI: 10.1016/j.jacc.2012.05.052
Quantification of absolute myocardial perfusion in patients with coronary artery disease: comparison between cardiovascular magnetic resonance and positron emission tomography
Abstract
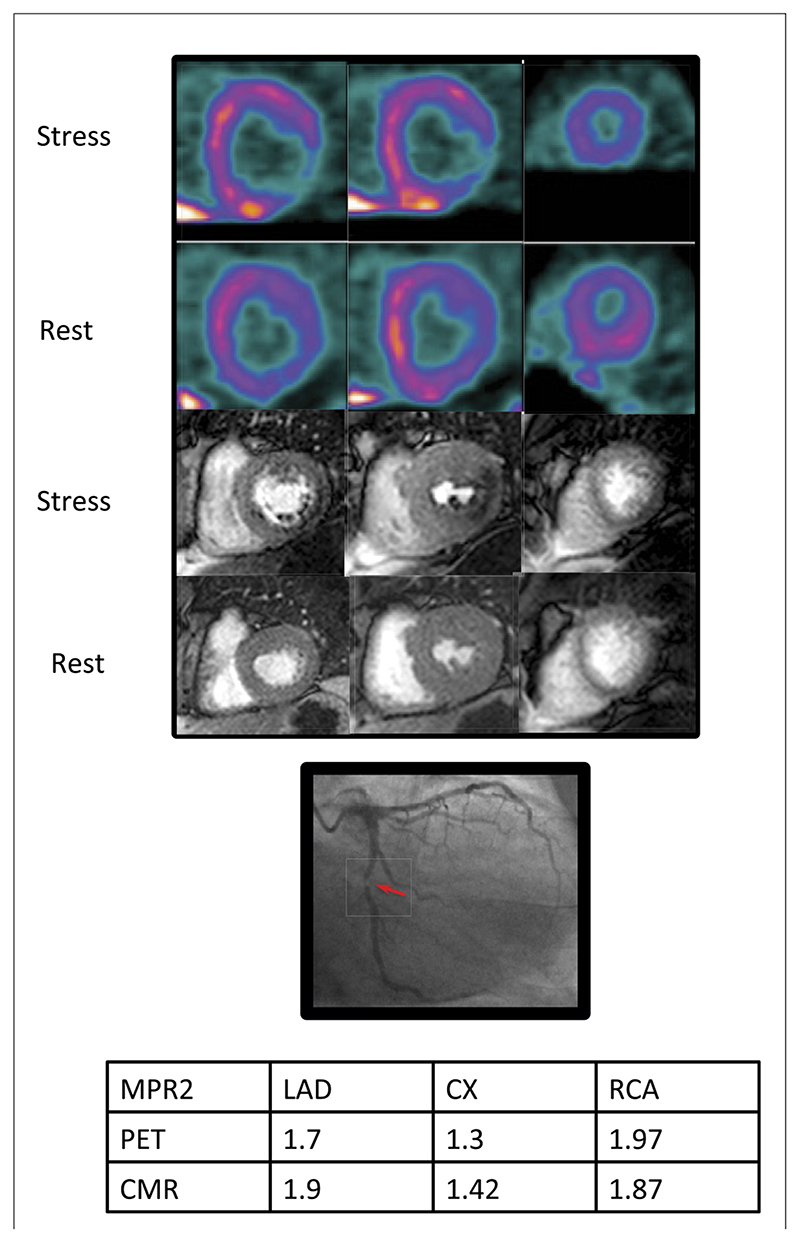
Objectives: The aim of this study was to compare fully quantitative cardiovascular magnetic resonance (CMR) and positron emission tomography (PET) myocardial perfusion and myocardial perfusion reserve (MPR) measurements in patients with coronary artery disease (CAD).
Background: Absolute quantification of myocardial perfusion and MPR with PET have proven diagnostic and prognostic roles in patients with CAD. Quantitative CMR perfusion imaging has been established more recently and has been validated against PET in normal hearts. However, there are no studies comparing fully quantitative CMR against PET perfusion imaging in patients with CAD.
Methods: Forty-one patients with known or suspected CAD prospectively underwent quantitative (13)N-ammonia PET and CMR perfusion imaging before coronary angiography.
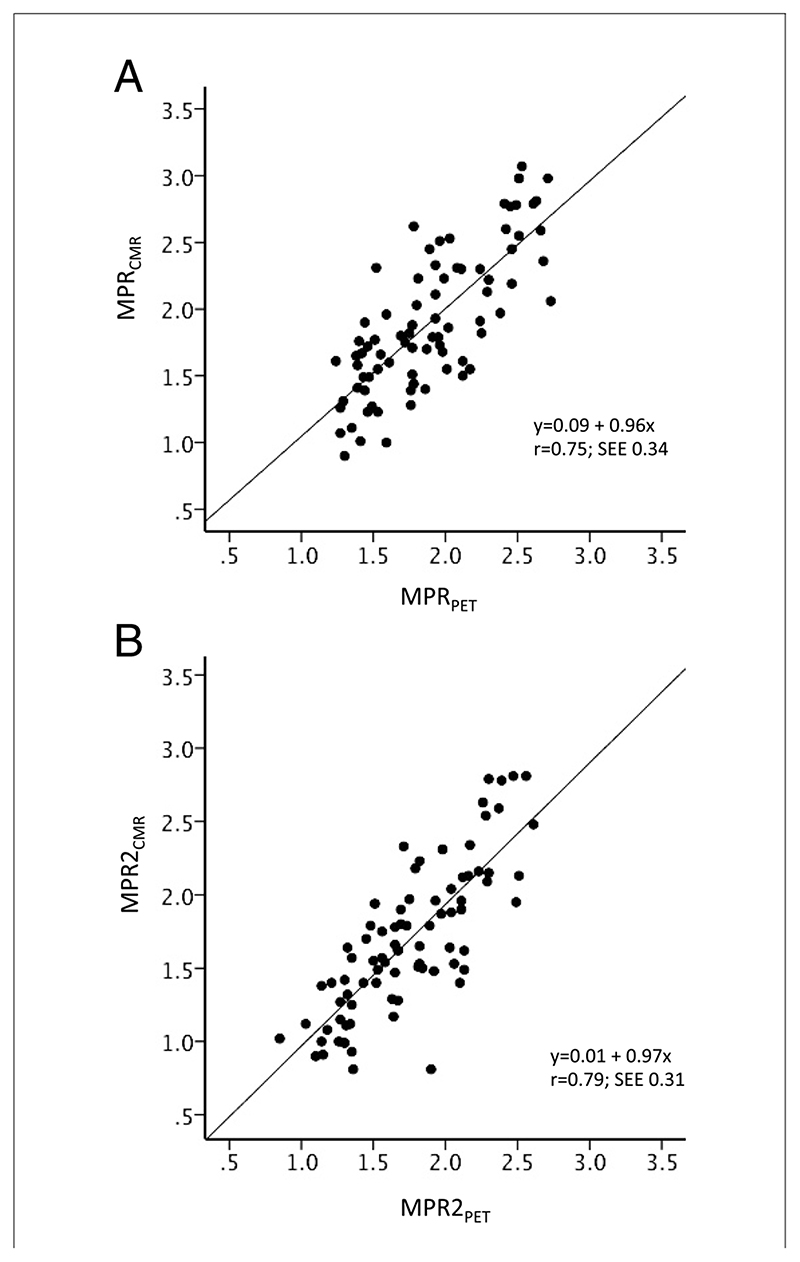
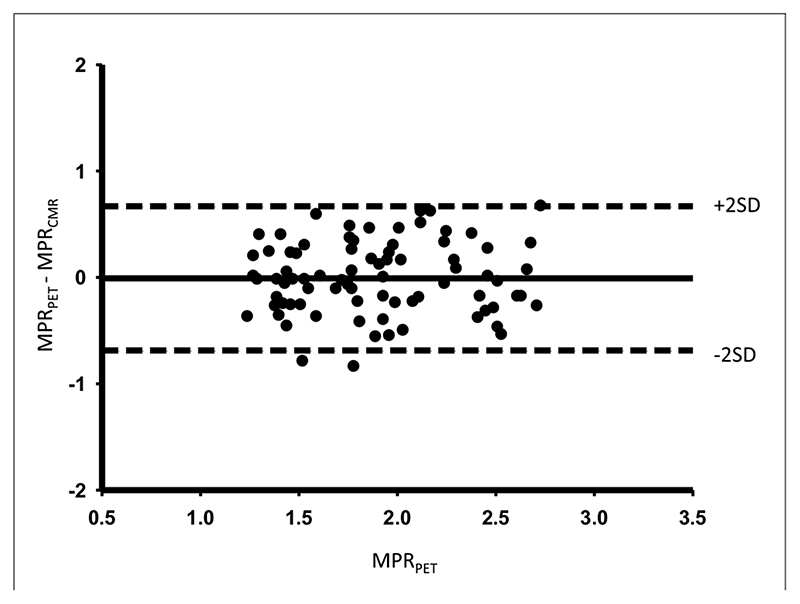
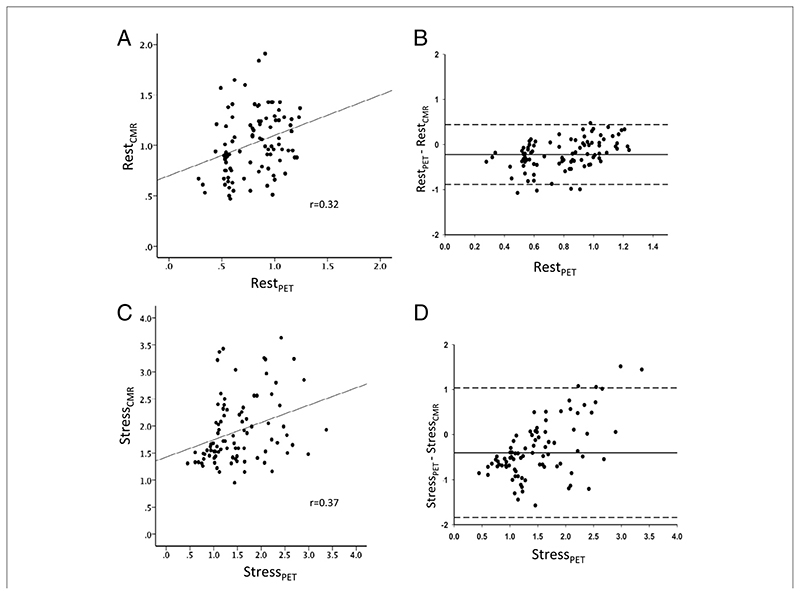
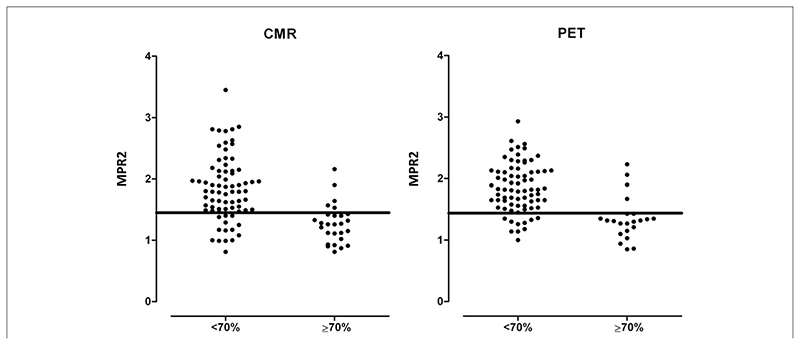
Results: The CMR-derived MPR (MPR(CMR)) correlated well with PET-derived measurements (MPR(PET)) (r = 0.75, p < 0.0001). MPR(CMR) and MPR(PET) for the 2 lowest scoring segments in each coronary territory also correlated strongly (r = 0.79, p < 0.0001). Absolute CMR perfusion values correlated significantly, but weakly, with PET values both at rest (r = 0.32; p = 0.002) and during stress (r = 0.37; p < 0.0001). Area under the receiver-operating characteristic curve for MPR(PET) to detect significant CAD was 0.83 (95% confidence interval: 0.73 to 0.94) and for MPR(CMR) was 0.83 (95% confidence interval: 0.74 to 0.92). An MPR(PET) ≤1.44 predicted significant CAD with 82% sensitivity and 87% specificity, and MPR(CMR) ≤1.45 predicted significant CAD with 82% sensitivity and 81% specificity.
Conclusions: There is good correlation between MPR(CMR) and MPR(PET.) For the detection of significant CAD, MPR(PET) and MPR(CMR) seem comparable and very accurate. However, absolute perfusion values from PET and CMR are only weakly correlated; therefore, although quantitative CMR is clinically useful, further refinements are still required.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Quantification of myocardial perfusion and myocardial perfusion reserve by positron emission tomography and cardiovascular magnetic resonance imaging.J Am Coll Cardiol. 2012 Oct 16;60(16):1556-7. doi: 10.1016/j.jacc.2012.05.051. Epub 2012 Sep 19. J Am Coll Cardiol. 2012. PMID: 22999721 No abstract available.
References
-
- Knuuti J, Kajander S, Mäki M, Ukkonen H. Quantification of myocardial blood flow will reform the detection of CAD. J Nucl Cardiol. 2009;16:497–506. - PubMed
-
- Kajander SA, Joutsiniemi E, Saraste M, et al. Clinical value of absolute quantification of myocardial perfusion with (15)O-water in coronary artery disease. Circ Cardiovasc Imaging. 2011;4:678–84. - PubMed
-
- Herzog BA, Husmann L, Valenta I, et al. Long-term prognostic value of 13N-ammonia myocardial perfusion positron emission tomography added value of coronary flow reserve. J Am Coll Cardiol. 2009;54:150–6. - PubMed
-
- Tio RA, Dabeshlim A, Siebelink H-MJ, et al. Comparison between the prognostic value of left ventricular function and myocardial perfusion reserve in patients with ischemic heart disease. J Nucl Med. 2009;50:214–9. - PubMed
-
- Camici PG, Crea F. Coronary microvascular dysfunction. N Engl J Med. 2007;356:830–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
