The effect of the US Medicare Part D coverage gaps on medication use among patients with depression and heart failure
- PMID: 23001279
- PMCID: PMC3471664
The effect of the US Medicare Part D coverage gaps on medication use among patients with depression and heart failure
Abstract
Background: Medication use among Medicare beneficiaries has increased and adherence has improved since the implementation of the Medicare Part D prescription drug benefit in 2006. However, the structure of the benefit, particularly, the coverage gap, is still problematic. It is critical to understand how beneficiaries with coexisting conditions respond to the coverage gap and whether their response differs by type of medications.
Aims of the study: The paper aims to evaluate the effects of Medicare Part D's coverage gap on drug regimens among beneficiaries with coexisting depression and heart failure (HF).
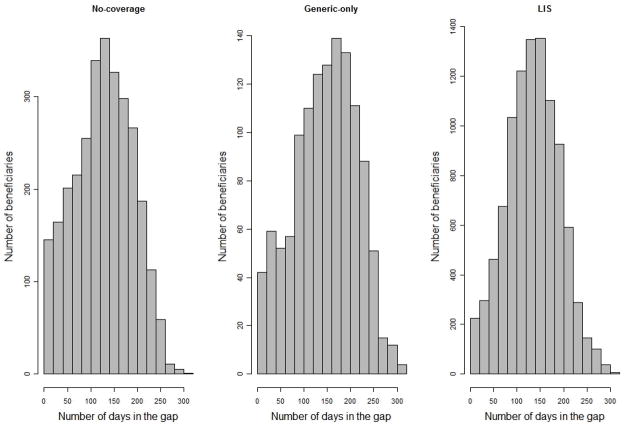
Methods: Drug utilization patterns and medication adherence of a 5% random sample of Medicare Part D beneficiaries with depression and HF in 2007 were observed. Drug utilization patterns were measured on the basis of reported drug claims and medication adherence was defined as the proportion of days of medication possession in a given period. We compared pre-post drug use patterns and medication adherence across three groups: no coverage, generic coverage, and full coverage due to low-income subsidies (LIS) and used propensity score weighting to adjust for difference across groups.
Results: Beneficiaries with some drug coverage in the gap were more likely to enter the gap: 82% for LIS, 79% for generic-only and 58% for no coverage. Beneficiaries without drug coverage reduced their use of antidepressants by 5.0% (95% CI 1.7%-8.2%), and HF drugs by 9.4% (95% CI 7.2%-11.5%) after they entered the coverage gap. Those with generic coverage cut their brand-name drugs more than generic drugs but did not shift to generic drugs. However, adherence to antidepressants did not change; adherence to HF drugs reduced slightly, 2.5% (95% CI 1.2%-3.7%) in the no-coverage group and 2.6% (95% CI 1.3%-3.9%) in the generic-coverage group.
Conclusions: The coverage gap was associated with a modest reduction in number of prescriptions filled for depression and HF but it was not associated with a significant effect on adherence.
Implications for health policy: We found that beneficiaries with coexisting depression and HF were less likely to reduce their drug use than beneficiaries in general. In addition, the gap was not associated with a large reduction in adherence. It suggests that concerns about the coverage gap's harmful effects on medication adherence, or comorbidities might be overstated.
Implications for further research: Further studies on how people make medication use decisions in the face of changes in benefits and how the coverage affects non-drug medical outcomes are warranted.
Figures
Comment in
-
The effect of the medication coverage gap on seniors with co-occurring depression and heart failure.J Ment Health Policy Econ. 2012 Sep;15(3):103-4. J Ment Health Policy Econ. 2012. PMID: 23012766 No abstract available.
References
-
- Centers for Medicare & Medicaid Services. Chronic Condition Data Warehouse User Guide: Version 1.8. 2011 [cited 2011 September 9]; Available from: http://www.ccwdata.org/cs/groups/public/documents/document/ccw_userguide....
-
- Regier DA, Narrow WE, Rae DS, Manderscheid RW, Locke BZ, Goodwin FK. The de facto US mental and addictive disorders service system. Epidemiologic catchment area prospective 1-year prevalence rates of disorders and services. Archives of General Psychiatry. 1993;50(2):85. - PubMed
-
- Melfi CA, Chawla AJ, Croghan TW, Hanna MP, Kennedy S, Sredl K. The effects of adherence to antidepressant treatment guidelines on relapse and recurrence of depression. Archives of General Psychiatry. 1998;55(12):1128. - PubMed
-
- Rutledge T, Reis VA, Linke SE, Greenberg BH, Mills PJ. Depression in heart failure a meta-analytic review of prevalence, intervention effects, and associations with clinical outcomes. J Am Coll Cardiol. 2006;48:1527–1537. - PubMed
-
- Sullivan M, Simon G, Spertus J, Russo J. Depression-related costs in heart failure care. Arch Intern Med. 2002;162:1860–1866. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous