

Systematic review and meta-analysis of safety of laparoscopic versus open appendicectomy for suspected appendicitis in pregnancy
- PMID: 23001791
- PMCID: PMC3494303
- DOI: 10.1002/bjs.8889
Systematic review and meta-analysis of safety of laparoscopic versus open appendicectomy for suspected appendicitis in pregnancy
Abstract
Background: Laparoscopic appendicectomy has gained wide acceptance as an alternative to open appendicectomy during pregnancy. However, data regarding the safety and optimal surgical approach to appendicitis in pregnancy are still controversial.
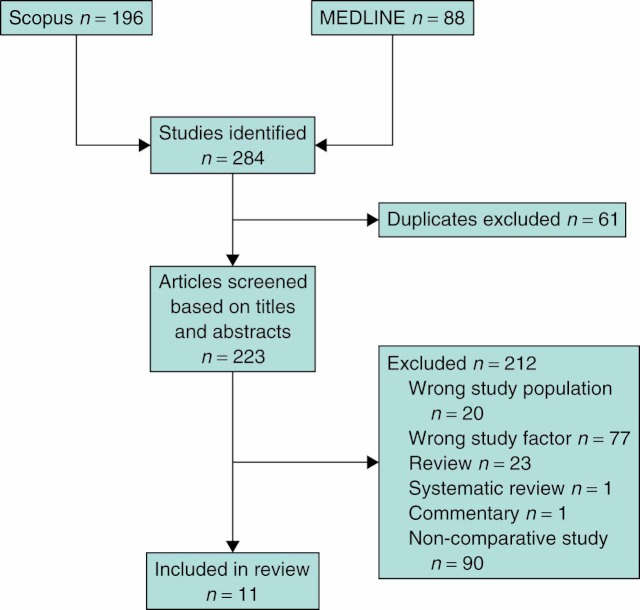
Methods: This was a systematic review and meta-analysis of studies comparing laparoscopic and open appendicectomy in pregnancy identified using PubMed and Scopus search engines from January 1990 to July 2011. Two reviewers independently extracted data on fetal loss, preterm delivery, wound infection, duration of operation, hospital stay, Apgar score and birth weight between laparoscopic and open appendicectomy groups.
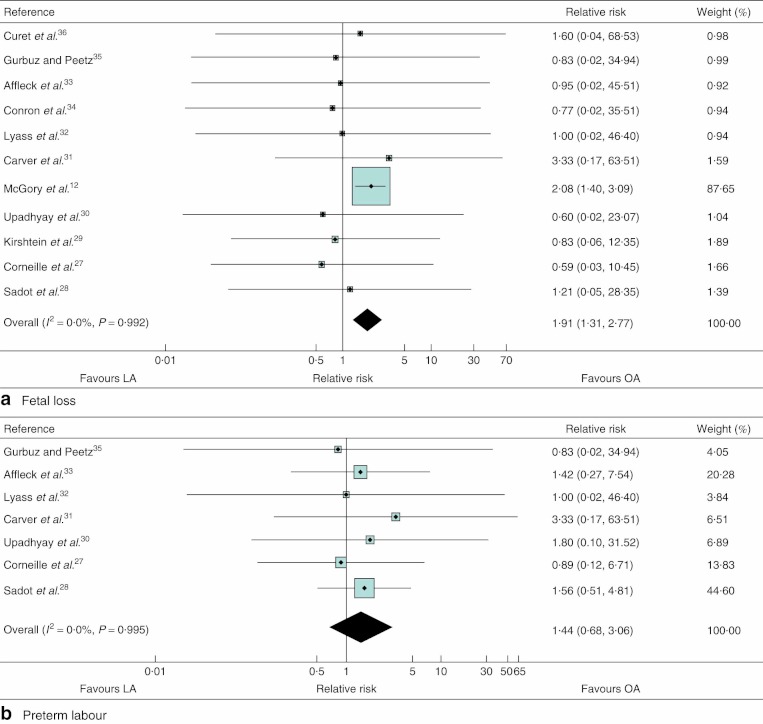
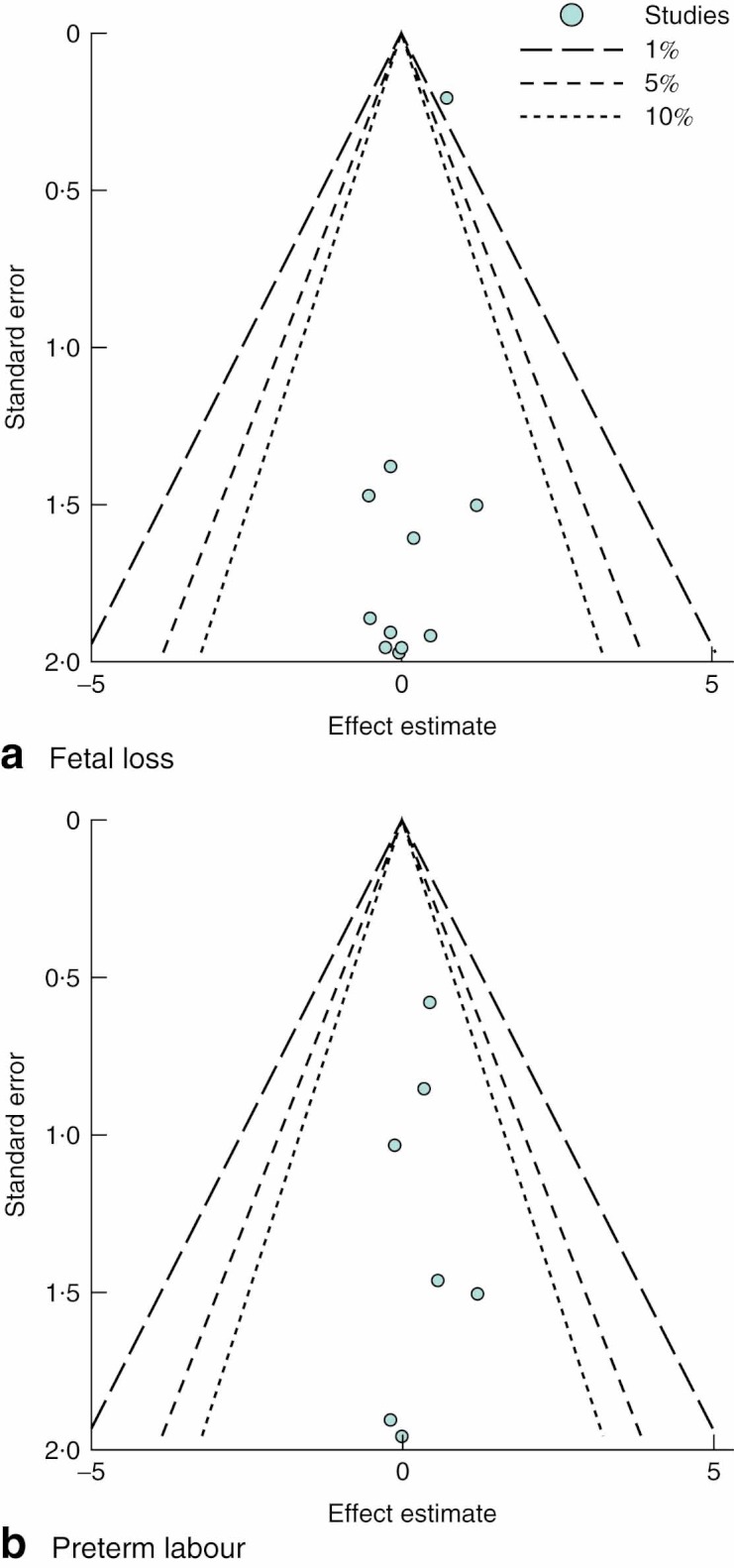
Results: Eleven studies with a total of 3415 women (599 in laparoscopic and 2816 in open group) were included in the analysis. Fetal loss was statistically significantly worse in those who underwent laparoscopy compared with open appendicectomy; the pooled relative risk (RR) was 1·91 (95 per cent confidence interval (c.i.) 1·31 to 2·77) without heterogeneity. The pooled RR for preterm labour was 1·44 (0·68 to 3·06), but this risk was not statistically significant. The mean difference in length of hospital stay was - 0·49 (-1·76 to - 0·78) days, but this was not clinically significant. No significant difference was found for wound infection, birth weight, duration of operation or Apgar score.
Conclusion: The available low-grade evidence suggests that laparoscopic appendicectomy in pregnant women might be associated with a greater risk of fetal loss.
Copyright © 2012 British Journal of Surgery Society Ltd. Published by John Wiley & Sons, Ltd.
Figures
Comment in
-
Systematic review and meta-analysis of safety of laparoscopic versus open appendicectomy for suspected appendicitis in pregnancy (Br J Surg 2012; 99: 1470-1478).Br J Surg. 2012 Nov;99(11):1478-9. doi: 10.1002/bjs.8890. Br J Surg. 2012. PMID: 23027069 No abstract available.
References
-
- Kort B, Katz VL, Watson WJ. The effect of nonobstetric operation during pregnancy. Surg Gynecol Obstet. 1993;177:371–376. - PubMed
-
- Gilo NB, Amini D, Landy HJ. Appendicitis and cholecystitis in pregnancy. Clin Obstet Gynecol. 2009;52:586–596. - PubMed
-
- Yilmaz HG, Akgun Y, Bac B, Celik Y. Acute appendicitis in pregnancy—risk factors associated with principal outcomes: a case control study. Int J Surg. 2007;5:192–197. - PubMed
-
- Ueberrueck T, Koch A, Meyer L, Hinkel M, Gastinger I. Ninety-four appendectomies for suspected acute appendicitis during pregnancy. World J Surg. 2004;28:508–511. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
