

Mirizzi syndrome: history, current knowledge and proposal of a simplified classification
- PMID: 23002333
- PMCID: PMC3442202
- DOI: 10.3748/wjg.v18.i34.4639
Mirizzi syndrome: history, current knowledge and proposal of a simplified classification
Abstract
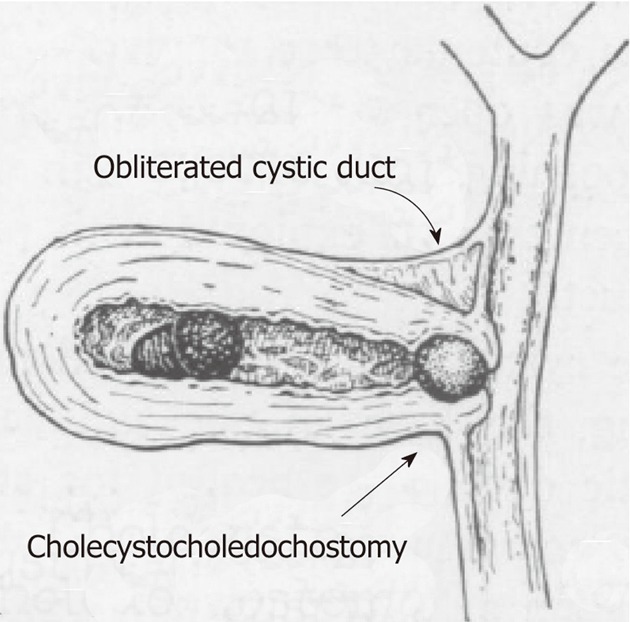
Chronic complications of symptomatic gallstone disease, such as Mirizzi syndrome, are rare in Western developed countries with an incidence of less than 1% a year. The importance and implications of this condition are related to their associated and potentially serious surgical complications such as bile duct injury, and to its modern management when encountered during laparoscopic cholecystectomy. The pathophysiological process leading to the subtypes of Mirizzi syndrome has been explained by means of a pressure ulcer caused by an impacted gallstone at the gallbladder infundibulum, leading to an inflammatory response causing first external obstruction of the bile duct, and eventually eroding into the bile duct and evolving to a cholecystocholedochal or cholecystohepatic fistula. This article reviews the life of Pablo Luis Mirizzi, describes the earlier and later descriptions of Mirizzi syndrome, discusses the pathophysiological process leading to the development of these uncommon fistulas, reviews the current diagnostic modalities and surgical approaches and finally proposes a simplified classification for Mirizzi syndrome intended to standardize the reports on this condition and to eventually develop a consensual surgical approach to this unexpected and seriously dangerous condition.
Keywords: Cholelithiasis; Chronic gallbladder disease; Gallstone disease; Mirizzi syndrome.
Figures




References
-
- Abou-Saif A, Al-Kawas FH. Complications of gallstone disease: Mirizzi syndrome, cholecystocholedochal fistula, and gallstone ileus. Am J Gastroenterol. 2002;97:249–254. - PubMed
-
- Dorrance HR, Lingam MK, Hair A, Oien K, O’Dwyer PJ. Acquired abnormalities of the biliary tract from chronic gallstone disease. J Am Coll Surg. 1999;189:269–273. - PubMed
-
- Corts MR, Vasquez AG. Frequency of the Mirizzi syndrome in a teaching hospital. Cir Gen. 2003;25:334–337.
-
- Beltran MA, Csendes A, Cruces KS. The relationship of Mirizzi syndrome and cholecystoenteric fistula: validation of a modified classification. World J Surg. 2008;32:2237–2243. - PubMed
-
- Kok KY, Goh PY, Ngoi SS. Management of Mirizzi’s syndrome in the laparoscopic era. Surg Endosc. 1998;12:1242–1244. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
