

Quality of ulcer healing in gastrointestinal tract: its pathophysiology and clinical relevance
- PMID: 23002355
- PMCID: PMC3447265
- DOI: 10.3748/wjg.v18.i35.4811
Quality of ulcer healing in gastrointestinal tract: its pathophysiology and clinical relevance
Abstract
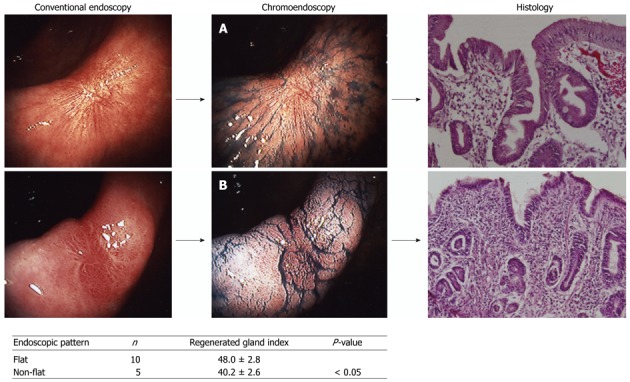
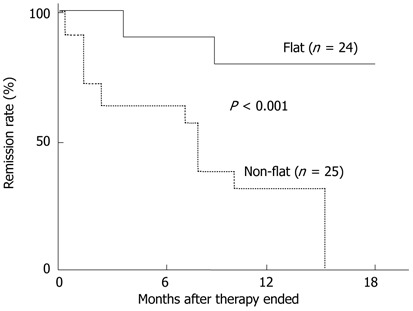
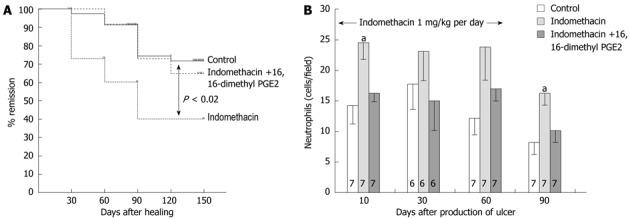
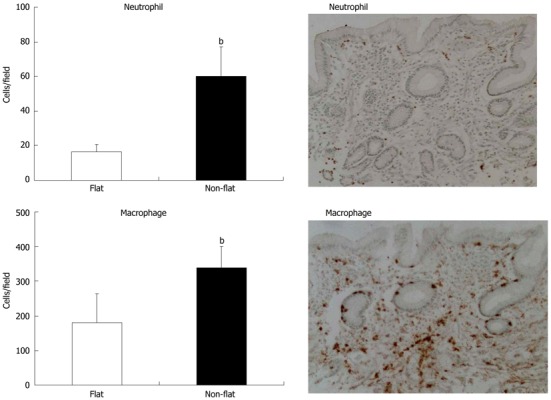
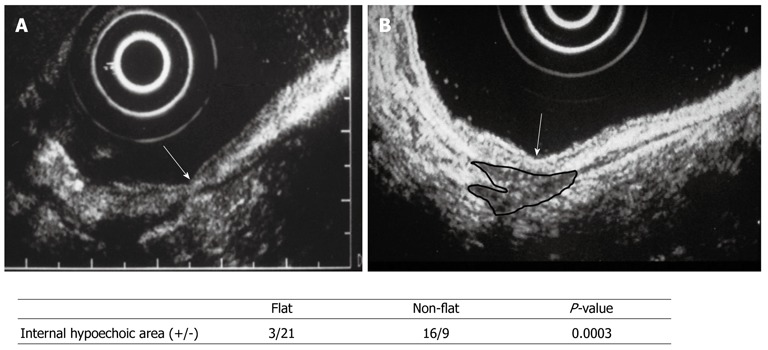
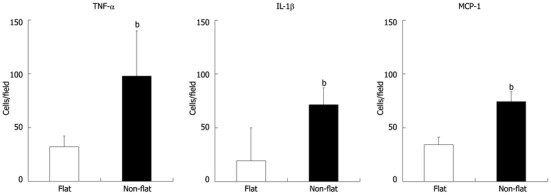
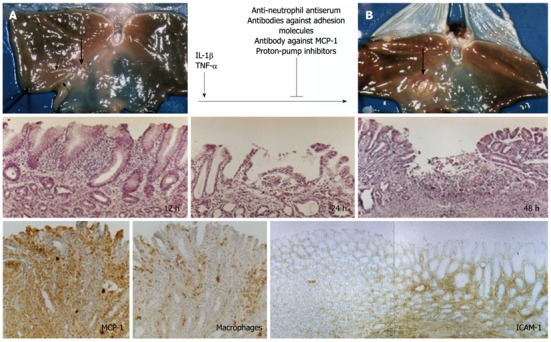
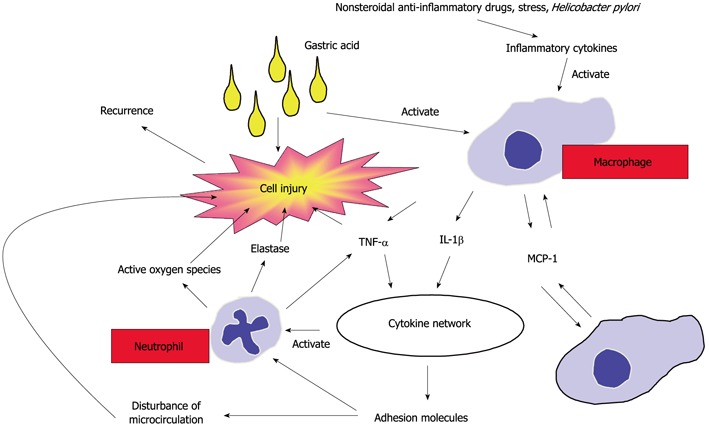
In this paper, we review the concept of quality of ulcer healing (QOUH) in the gastrointestinal tract and its role in the ulcer recurrence. In the past, peptic ulcer disease (PUD) has been a chronic disease with a cycle of repeated healing/remission and recurrence. The main etiological factor of PUD is Helicobacter pylori (H. pylori), which is also the cause of ulcer recurrence. However, H. pylori-negative ulcers are present in 12%-20% of patients; they also recur and are on occasion intractable. QOUH focuses on the fact that mucosal and submucosal structures within ulcer scars are incompletely regenerated. Within the scars of healed ulcers, regenerated tissue is immature and with distorted architecture, suggesting poor QOUH. The abnormalities in mucosal regeneration can be the basis for ulcer recurrence. Our studies have shown that persistence of macrophages in the regenerated area plays a key role in ulcer recurrence. Our studies in a rat model of ulcer recurrence have indicated that proinflammatory cytokines trigger activation of macrophages, which in turn produce increased amounts of cytokines and chemokines, which attract neutrophils to the regenerated area. Neutrophils release proteolytic enzymes that destroy the tissue, resulting in ulcer recurrence. Another important factor in poor QOUH can be deficiency of endogenous prostaglandins and a deficiency and/or an imbalance of endogenous growth factors. Topically active mucosal protective and antiulcer drugs promote high QOUH and reduce inflammatory cell infiltration in the ulcer scar. In addition to PUD, the concept of QOUH is likely applicable to inflammatory bowel diseases including Crohn's disease and ulcerative colitis.
Keywords: Cytokines; Growth factors; Peptic ulcer disease; Prostaglandin; Quality of ulcer healing; Recurrence.
Figures
References
-
- Arakawa T, Higuchi K, Fujiwara Y, Tominaga K, Watanabe T, Shiba M, Uchida T, Kuroki T. Helicobacter pylori: criminal or innocent bystander? J Gastroenterol. 2000;35 Suppl 12:42–46. - PubMed
-
- Jang HJ, Choi MH, Shin WG, Kim KH, Chung YW, Kim KO, Park CH, Baek IH, Baik KH, Kae SH, et al. Has peptic ulcer disease changed during the past ten years in Korea? A prospective multi-center study. Dig Dis Sci. 2008;53:1527–1531. - PubMed
-
- Musumba C, Jorgensen A, Sutton L, Van Eker D, Moorcroft J, Hopkins M, Pritchard DM, Pirmohamed M. The relative contribution of NSAIDs and Helicobacter pylori to the aetiology of endoscopically-diagnosed peptic ulcer disease: observations from a tertiary referral hospital in the UK between 2005 and 2010. Aliment Pharmacol Ther. 2012;36:48–56. - PubMed
-
- Sbrozzi-Vanni A, Zullo A, Di Giulio E, Hassan C, Corleto VD, Lahner E, Annibale B. Low prevalence of idiopathic peptic ulcer disease: an Italian endoscopic survey. Dig Liver Dis. 2010;42:773–776. - PubMed
-
- Kang JM, Seo PJ, Kim N, Lee BH, Kwon J, Lee DH, Jung HC. Analysis of direct medical care costs of peptic ulcer disease in a Korean tertiary medical center. Scand J Gastroenterol. 2012;47:36–42. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
