

Analysis of colonoscopic perforations at a local clinic and a tertiary hospital
- PMID: 23002362
- PMCID: PMC3447272
- DOI: 10.3748/wjg.v18.i35.4898
Analysis of colonoscopic perforations at a local clinic and a tertiary hospital
Abstract
Aim: To define the clinical characteristics, and to assess the management of colonoscopic complications at a local clinic.
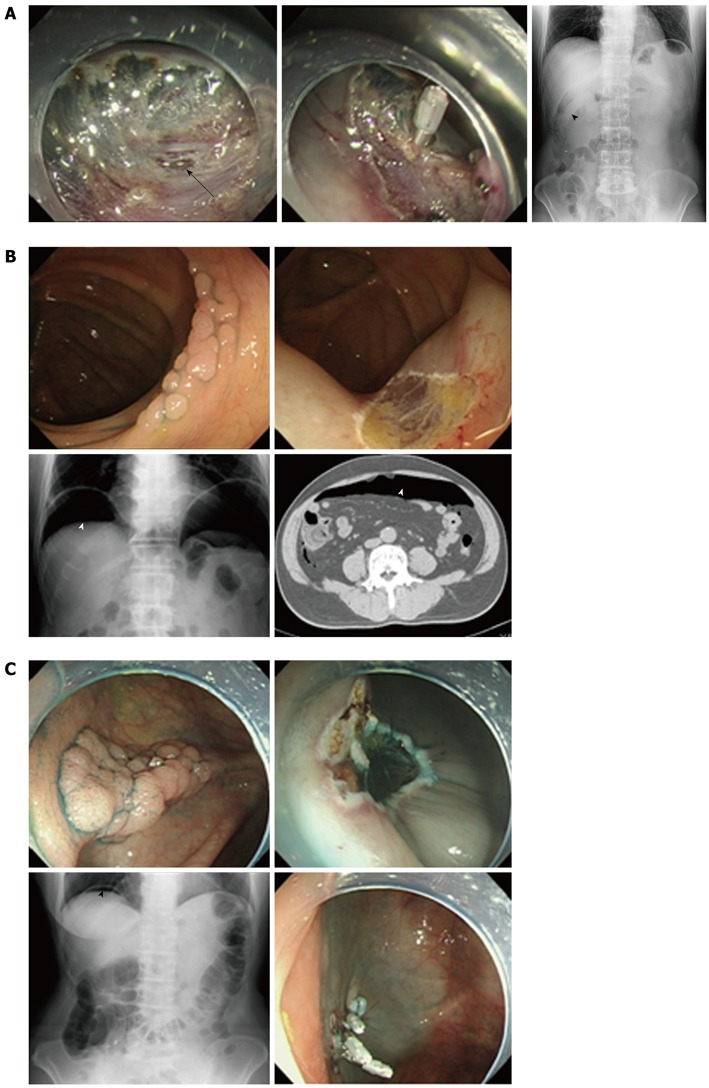
Methods: A retrospective review of the medical records was performed for the patients with iatrogenic colon perforations after endoscopy at a local clinic between April 2006 and December 2010. Data obtained from a tertiary hospital in the same region were also analyzed. The underlying conditions, clinical presentations, perforation locations, treatment types (operative or conservative) and outcome data for patients at the local clinic and the tertiary hospital were compared.
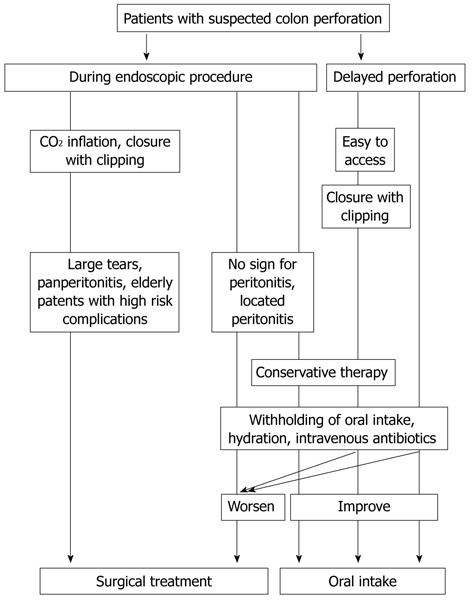
Results: A total of 10 826 colonoscopies, and 2625 therapeutic procedures were performed at a local clinic and 32 148 colonoscopies, and 7787 therapeutic procedures were performed at the tertiary hospital. The clinic had no perforations during diagnostic colonoscopy and 8 (0.3%) perforations were determined to be related to therapeutic procedures. The perforation rates in each therapeutic procedure were 0.06% (1/1609) in polypectomy, 0.2% (2/885) in endoscopic mucosal resection (EMR), and 3.8% (5/131) in endoscopic submucosal dissection (ESD). Perforation rates for ESD were significantly higher than those for polypectomy or EMR (P < 0.01). All of these patients were treated conservatively. On the other hand, three (0.01%) perforation cases were observed among the 24 361 diagnostic procedures performed, and these cases were treated with surgery in a tertiary hospital. Six perforations occurred with therapeutic endoscopy (perforation rate, 0.08%; 1 per 1298 procedures). Perforation rates for specific procedure types were 0.02% (1 per 5500) for polypectomy, 0.17% (1 per 561) for EMR, 2.3% (1 per 43) for ESD in the tertiary hospital. There were no differences in the perforation rates for each therapeutic procedure between the clinic and the tertiary hospital. The incidence of iatrogenic perforation requiring surgical treatment was quite low in both the clinic and the tertiary hospital. No procedure-related mortalities occurred. Performing closure with endoscopic clipping reduced the C-reactive protein (CRP) titers. The mean maximum CRP titer was 2.9 ± 1.6 mg/dL with clipping and 9.7 ± 6.2 mg/dL without clipping, respectively (P < 0.05). An operation is indicated in the presence of a large perforation, and in the setting of generalized peritonitis or ongoing sepsis. Although we did not experience such case in the clinic, patients with large perforations should be immediately transferred to a tertiary hospital. Good relationships between local clinics and nearby tertiary hospitals should therefore be maintained.
Conclusion: It was therefore found to be possible to perform endoscopic treatment at a local clinic when sufficient back up was available at a nearby tertiary hospital.
Keywords: Colon perforation; Colonoscopy; Endoscopic clipping; Endoscopic mucosal resection; Endoscopic submucosal dissection; Polypectomy.
Figures
Similar articles
-
Incidence and management of colonoscopic perforations in Korea.Digestion. 2008;78(4):218-23. doi: 10.1159/000190811. Epub 2009 Jan 13. Digestion. 2008. PMID: 19142003
-
Iatrogenic perforation associated with therapeutic colonoscopy: a multicenter study in Japan.J Gastroenterol Hepatol. 2007 Sep;22(9):1409-14. doi: 10.1111/j.1440-1746.2007.05022.x. Epub 2007 Jun 25. J Gastroenterol Hepatol. 2007. PMID: 17593224
-
Lower rate of colonoscopic perforation: 110,785 patients of colonoscopy performed by colorectal surgeons in a large teaching hospital in China.Surg Endosc. 2014 Aug;28(8):2309-16. doi: 10.1007/s00464-014-3458-1. Epub 2014 Feb 25. Surg Endosc. 2014. PMID: 24566747
-
Colonoscopic perforations: a review of 30,366 patients.Surg Endosc. 2007 Jun;21(6):994-7. doi: 10.1007/s00464-007-9251-7. Epub 2007 Apr 24. Surg Endosc. 2007. PMID: 17453289 Review.
-
Our experience with endoscopic repair of large colonoscopic perforations and review of the literature.Tech Coloproctol. 2008 Dec;12(4):315-21; discussion 322. doi: 10.1007/s10151-008-0442-6. Epub 2008 Nov 18. Tech Coloproctol. 2008. PMID: 19018468 Review.
Cited by
-
Complications, Implications, and Prevention of Electrosurgical Injuries: Corner Stone of Diathermy Use for Junior Surgical Trainees.Surg J (N Y). 2017 Sep 14;3(4):e148-e153. doi: 10.1055/s-0037-1606547. eCollection 2017 Oct. Surg J (N Y). 2017. PMID: 28924615 Free PMC article. Review.
-
Laparoscopic Primary Colorrhaphy for Acute Iatrogenic Perforations during Colonoscopy.Minim Invasive Surg. 2013;2013:823506. doi: 10.1155/2013/823506. Epub 2013 Feb 7. Minim Invasive Surg. 2013. PMID: 23476761 Free PMC article.
-
Endoscopic submucosal dissection vs endoscopic mucosal resection for colorectal polyps: A meta-analysis and meta-regression with single arm analysis.World J Gastroenterol. 2021 Jul 7;27(25):3925-3939. doi: 10.3748/wjg.v27.i25.3925. World J Gastroenterol. 2021. PMID: 34321855 Free PMC article.
-
Outcome, comorbidity, hospitalization and 30-day mortality after closure of acute perforations and postoperative anastomotic leaks by the over-the-scope clip (OTSC) in an unselected cohort of patients.Surg Endosc. 2017 Jun;31(6):2411-2425. doi: 10.1007/s00464-016-5242-x. Epub 2016 Sep 15. Surg Endosc. 2017. PMID: 27633439
-
Endoscopic Management of the Ascending Colon Perforation Secondary to a Rare-Earth Magnets Ingestion in a Pediatric Patient.ACG Case Rep J. 2020 Aug 10;7(8):e00436. doi: 10.14309/crj.0000000000000436. eCollection 2020 Aug. ACG Case Rep J. 2020. PMID: 32821766 Free PMC article.
References
-
- Forde KA. Colonoscopic screening for colon cancer. Surg Endosc. 2006;20 Suppl 2:S471–S474. - PubMed
-
- Juillerat P, Peytremann-Bridevaux I, Vader JP, Arditi C, Schusselé Filliettaz S, Dubois RW, Gonvers JJ, Froehlich F, Burnand B, Pittet V. Appropriateness of colonoscopy in Europe (EPAGE II). Presentation of methodology, general results, and analysis of complications. Endoscopy. 2009;41:240–246. - PubMed
-
- Hachisu T. Evaluation of endoscopic hemostasis using an improved clipping apparatus. Surg Endosc. 1988;2:13–17. - PubMed
-
- Hagel AF, Boxberger F, Dauth W, Kessler HP, Neurath MF, Raithel M. Colonoscopy-associated perforation: a 7-year survey of in-hospital frequency, treatment and outcome in a German university hospital. Colorectal Dis. 2012;14:1121–1125. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
