

Protecting the infant brain during cardiac surgery: a systematic review
- PMID: 23006704
- PMCID: PMC4249676
- DOI: 10.1016/j.athoracsur.2012.05.135
Protecting the infant brain during cardiac surgery: a systematic review
Abstract
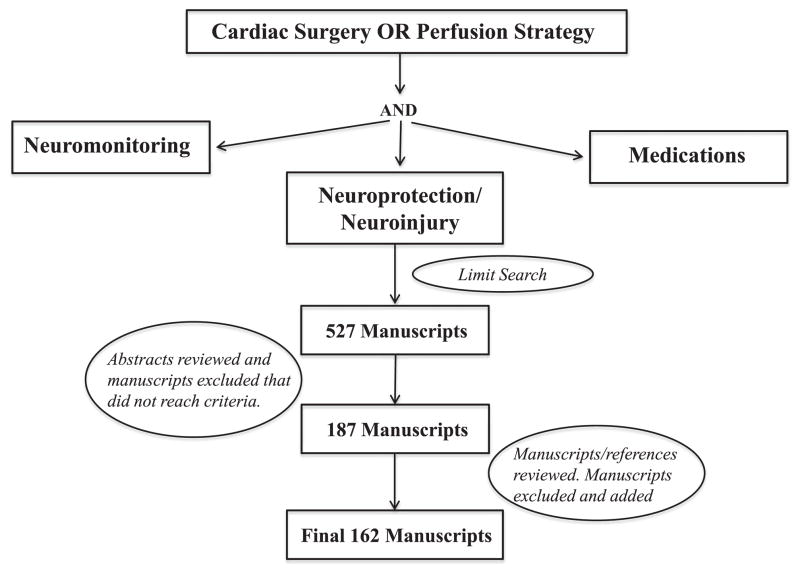
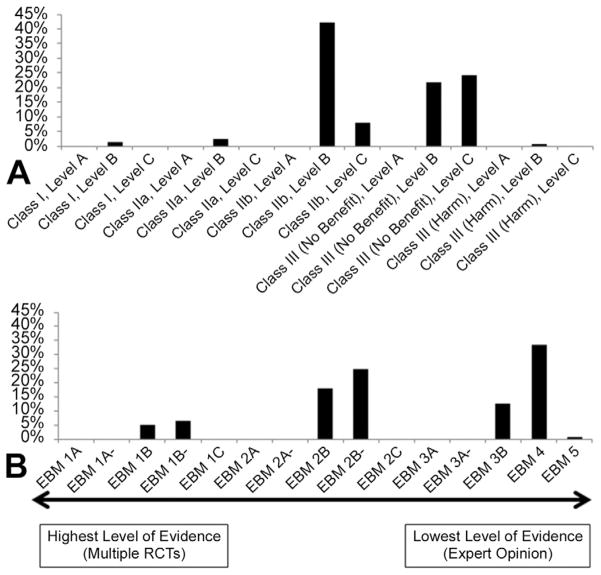
Prevention of brain injury during congenital heart surgery has focused on intraoperative and perioperative neuroprotection and neuromonitoring. Many strategies have been adopted as "standard of care." However, the strength of evidence for these practices and the relationship to long-term outcomes are unknown. We performed a systematic review (January 1, 1990 to July 30, 2010) of neuromonitoring and neuroprotection strategies during cardiopulmonary bypass (CPB) in infants of age 1 year or less. Papers were graded individually and as thematic groups, assigning evidence-based medicine and American College of Cardiology/American Heart Association (ACC/AHA) level of evidence grades. Consensus scores were determined by adjudication. Literature search identified 527 manuscripts; 162 met inclusion criteria. Study designs were prospective observational cohort (53.7%), case-control (21.6%), randomized clinical trial (13%), and retrospective observational cohort (9.9%). Median sample size was 43 (range 3 to 2,481). Primary outcome was evidence of structural brain injury or functional disability (neuroimaging, electroencephalogram, formal neurologic examination, or neurodevelopmental testing) in 43%. Follow-up information was reported in only 29%. The most frequent level of evidence was evidence-based medicine level 4 (33.3%) or ACC/AHA class IIB: level B (42%). The only intervention with sufficient evidence to recommend "the procedure or treatment should be performed" was avoidance of extreme hemodilution during CPB. Data supporting use of current neuromonitoring and neuroprotective techniques are limited. The level of evidence is insufficient to support effectiveness of most of these strategies. Well-designed studies with correlation to clinical outcomes and long-term follow-up are needed to develop guidelines for neuromonitoring and neuroprotection during CPB in infants.
Copyright © 2012 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Pulmonary artery perfusion versus no perfusion during cardiopulmonary bypass for open heart surgery in adults.Cochrane Database Syst Rev. 2018 Feb 8;2(2):CD011098. doi: 10.1002/14651858.CD011098.pub2. Cochrane Database Syst Rev. 2018. PMID: 29419895 Free PMC article.
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Effectiveness and safety of vitamin D in relation to bone health.Evid Rep Technol Assess (Full Rep). 2007 Aug;(158):1-235. Evid Rep Technol Assess (Full Rep). 2007. PMID: 18088161 Free PMC article.
-
Behavioral interventions to reduce risk for sexual transmission of HIV among men who have sex with men.Cochrane Database Syst Rev. 2008 Jul 16;(3):CD001230. doi: 10.1002/14651858.CD001230.pub2. Cochrane Database Syst Rev. 2008. PMID: 18646068
-
What is the value of routinely testing full blood count, electrolytes and urea, and pulmonary function tests before elective surgery in patients with no apparent clinical indication and in subgroups of patients with common comorbidities: a systematic review of the clinical and cost-effective literature.Health Technol Assess. 2012 Dec;16(50):i-xvi, 1-159. doi: 10.3310/hta16500. Health Technol Assess. 2012. PMID: 23302507 Free PMC article.
Cited by
-
Optimizing Neurodevelopmental Outcomes in Neonates With Congenital Heart Disease.Pediatrics. 2022 Nov 1;150(Suppl 2):e2022056415L. doi: 10.1542/peds.2022-056415L. Pediatrics. 2022. PMID: 36317967 Free PMC article.
-
Increased cerebral mitochondrial dysfunction and reactive oxygen species with cardiopulmonary bypass.Eur J Cardiothorac Surg. 2021 Jun 14;59(6):1256-1264. doi: 10.1093/ejcts/ezaa439. Eur J Cardiothorac Surg. 2021. PMID: 33367535 Free PMC article.
-
International Pediatric Perfusion Practice: 2016 Survey Results.J Extra Corpor Technol. 2021 Mar;53(1):7-26. doi: 10.1182/ject-2000033. J Extra Corpor Technol. 2021. PMID: 33814602 Free PMC article.
-
Effects of circulatory arrest and cardiopulmonary bypass on cerebral autoregulation in neonatal swine.Pediatr Res. 2022 May;91(6):1374-1382. doi: 10.1038/s41390-021-01525-3. Epub 2021 May 4. Pediatr Res. 2022. PMID: 33947997 Free PMC article.
-
Perioperative Management of a Child with Hypoplastic Left Heart Syndrome of the Jehovah's Witness Faith Presenting for Hybrid Comprehensive Stage II Procedure.J Extra Corpor Technol. 2016 Sep;48(3):141-147. J Extra Corpor Technol. 2016. PMID: 27729708 Free PMC article.
References
-
- Columb MO, Lalkhen A-G. Systematic reviews and meta-analyses. Current Anaesthesia & Critical Care. 2005;16:391–4.
-
- Nightingale A. A guide to systematic literature reviews. Surgery (Oxford) 2009;27:381–4.
-
- Pigula FA, Nemoto EM, Griffith BP, Siewers RD. Regional low-flow perfusion provides cerebral circulatory support during neonatal aortic arch reconstruction. J Thorac Cardiovasc Surg. 2000;119:331–9. - PubMed
-
- Newburger JW, Jonas RA, Wernovsky G, et al. A comparison of the perioperative neurologic effects of hypothermic circulatory arrest versus low-flow cardiopulmonary bypass in infant heart surgery. N Engl J Med. 1993;329:1057–64. - PubMed
-
- Kern FH, Ungerleider RM, Reves JG, et al. Effect of altering pump flow rate on cerebral blood flow and metabolism in infants and children. Ann Thorac Surg. 1993;56:1366–72. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
