

Microalbuminuria indicates long-term vascular risk in patients after acute stroke undergoing in-patient rehabilitation
- PMID: 23007013
- PMCID: PMC3517490
- DOI: 10.1186/1471-2377-12-102
Microalbuminuria indicates long-term vascular risk in patients after acute stroke undergoing in-patient rehabilitation
Abstract
Background: Patients in neurologic in-patient rehabilitation are at risk of cardio- and cerebrovascular events. Microalbuminuria (MAU) is frequent and an important risk predictor but has not been validated in in-patient rehabilitation. We therefore aimed to examine MAU as an indicator of risk and predictor of vascular events in a prospective study.
Methods: The INSIGHT (INvestigation of patients with ischemic Stroke In neuroloGic reHabiliTation) registry is the first to provide large scale data on 1,167 patients with acute stroke (< 3 months) that survived the initial phase of high risk and were undergoing neurologic in-patient rehabilitation. MAU was determined by dipstick-testing and correlated to baseline clinical variables (stroke-origin, functional impairment, co-morbidity, ankle-brachial-index, intima-media-thickeness) as well as vascular events after one year of follow-up. Comparisons were made with the χ2 or Mann-Whitney-U Test. Relative risks (RR) with 95% confidence intervals (CI) were estimated using log-binominal models. To evaluate the association between MAU and new vascular events as well as mortality, we calculated hazard ratios (HR) using Cox proportional hazard regression.
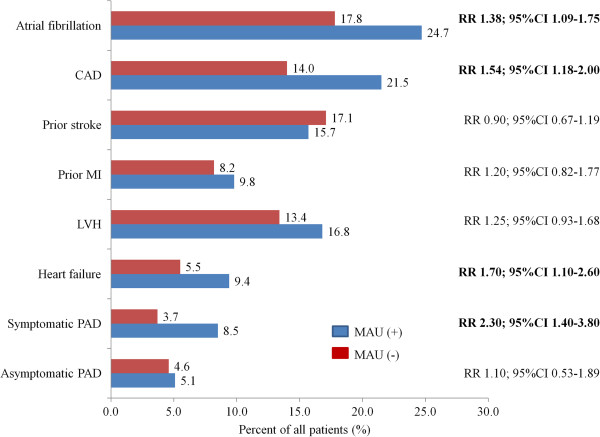
Results: A substantial proportion of patients was MAU positive at baseline (33.1%). Upon univariate analysis these patients were about 4 years older (69 vs. 65 years; p < 0.0001), had a slightly higher body mass index (27.8 vs. 27.1 kg/m2; p = 0.03) and increased waist circumference (79.5 vs. 50.4% for women [p < 0.0001] and 46.8 vs. 43.2% for men [p = 0.04]) and twice as often had diabetes mellitus (41.8 vs. 20.1%; p < 0.0001). Patients with MAU had a similar NIH stroke scale score (median 3 vs. 3; p = 0.379) but had lower values on the Barthel Index (median 75 vs. 90; p < 0.001). They had higher rates of atrial fibrillation (RR 1.38; 95% CI 1.09-1.75), coronary artery disease (RR 1.54; 95% CI 1.18-2.00), heart failure (RR 1.70; 95% CI 1.10-2.60) symptomatic peripheral artery disease (RR 2.30; 95% CI 1.40-3.80) and atherosclerotic stroke etiology (53.7 vs. 35.4%; p < 0.0001). MAU was associated with an increased intima-media-thickness, decreased ankle-brachial-index and polyvascular disease (RR 1.56; 95%CI 1.31-1.99). The event rate after a median follow-up of 13 months was 6.7% for fatal or nonfatal stroke, 4.7% for death, and 10.9% for combined vascular events (stroke, MI, vascular death). The presence of MAU was predictive for vascular events during the following year (HR for total mortality 2.2; 95% CI 1.3-3.7; HR for cardiovascular events 2.3; 95% 1.2 - 4.4).
Conclusions: INSIGHT demonstrated a significant association between MAU and polyvascular disease and further supports previous findings that MAU predicts cardio-/cerebrovascular events in patients recovering from ischemic stroke. This biomarker may also be used in patients during neurologic in-patient rehabilitation, opening a window of opportunity for early intervention in this patient group at increased risk for recurrent events.
Figures
References
-
- Ravera M, Ratto E, Vettoretti S, Viazzi F, Leoncini G, Parodi D, Tomolillo C, Del Sette M, Maviglio N, Deferrari G. et al.Microalbuminuria and subclinical cerebrovascular damage in essential hypertension. J Nephrol. 2002;15(5):519–524. - PubMed
-
- Ovbiagele B. Microalbuminuria: risk factor and potential therapeutic target for stroke? J Neurol Sci. 2008;271(1–2):21–28. - PubMed
-
- Yuyun MF, Khaw KT, Luben R, Welch A, Bingham S, Day NE, Wareham NJ. Microalbuminuria and stroke in a British population: the European Prospective Investigation into Cancer in Norfolk (EPIC-Norfolk) population study. J Intern Med. 2004;255(2):247–256. doi: 10.1046/j.1365-2796.2003.01264.x. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
