

Body mass index following natural menopause and hysterectomy with and without bilateral oophorectomy
- PMID: 23007036
- PMCID: PMC3530639
- DOI: 10.1038/ijo.2012.164
Body mass index following natural menopause and hysterectomy with and without bilateral oophorectomy
Abstract
Objective: The directional and temporal nature of relationships between overweight and obesity and hysterectomy with or without oophorectomy is not well understood. Overweight and obesity may be both a risk factor for the indications for these surgeries and a possible consequence of the procedure. We used prospective data to examine whether body mass index (BMI) increased more following hysterectomy with and without bilateral oophorectomy compared with natural menopause among middle-aged women.
Methods: BMI was assessed annually for up to 10 years in the Study of Women's Health Across the Nation (SWAN (n=1962)). Piecewise linear mixed growth models were used to examine changes in BMI before and after natural menopause, hysterectomy with ovarian conservation and hysterectomy with bilateral oophorectomy. Covariates included education, race/ethnicity, menopausal status, physical activity, self-rated health, hormone therapy use, antidepressant use, age and visit before the final menstrual period (FMP; for natural menopause) or surgery (for hysterectomy/oophorectomy).
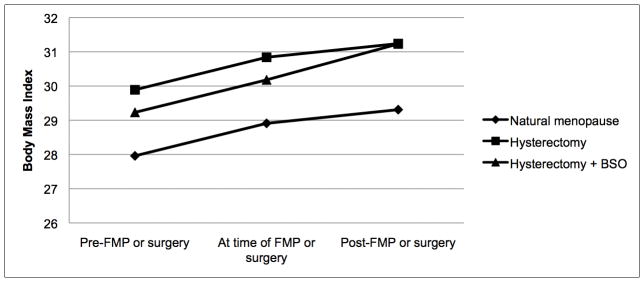
Results: By visit 10, 1780 (90.6%) women reached natural menopause, 106 (5.5%) reported hysterectomy with bilateral oophorectomy and 76 (3.9%) reported hysterectomy with ovarian conservation. In fully adjusted models, BMI increased for all women from baseline to FMP or surgery (annual rate of change=0.19 kg m(-2) per year), with no significant differences in BMI change between groups. BMI also increased for all women following FMP, but increased more rapidly in women following hysterectomy with bilateral oophorectomy (annual rate of change=0.21 kg m(-2) per year) as compared with following natural menopause (annual rate of change=0.08 kg m(-2) per year, P=0.03).
Conclusion: In this prospective examination, hysterectomy with bilateral oophorectomy was associated with greater increases in BMI in the years following surgery than following hysterectomy with ovarian conservation or natural menopause. This suggests that accelerated weight gain follows bilateral oophorectomy among women in midlife, which may increase risk for obesity-related chronic diseases.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Mood symptoms after natural menopause and hysterectomy with and without bilateral oophorectomy among women in midlife.Obstet Gynecol. 2012 May;119(5):935-41. doi: 10.1097/AOG.0b013e31824f9c14. Obstet Gynecol. 2012. PMID: 22525904 Free PMC article.
-
Changes in cardiovascular risk factors by hysterectomy status with and without oophorectomy: Study of Women's Health Across the Nation.J Am Coll Cardiol. 2013 Jul 16;62(3):191-200. doi: 10.1016/j.jacc.2013.04.042. Epub 2013 May 15. J Am Coll Cardiol. 2013. PMID: 23684687 Free PMC article.
-
The association of hysterectomy with or without ovarian conservation with subclinical atherosclerosis progression in healthy postmenopausal women.Menopause. 2023 Jul 1;30(7):692-702. doi: 10.1097/GME.0000000000002192. Epub 2023 May 16. Menopause. 2023. PMID: 37192828 Free PMC article. Clinical Trial.
-
Effect of bilateral oophorectomy on women's long-term health.Womens Health (Lond). 2009 Sep;5(5):565-76. doi: 10.2217/whe.09.42. Womens Health (Lond). 2009. PMID: 19702455 Review.
-
Should the ovaries be removed or retained at the time of hysterectomy for benign disease?Hum Reprod Update. 2010 Mar-Apr;16(2):131-41. doi: 10.1093/humupd/dmp037. Epub 2009 Sep 30. Hum Reprod Update. 2010. PMID: 19793841 Review.
Cited by
-
Women's Reproductive History and Pre-Clinical Peripheral Arterial Disease in Late Life: The San Diego Population Study.J Womens Health (Larchmt). 2019 Aug;28(8):1105-1115. doi: 10.1089/jwh.2018.7080. Epub 2018 Dec 1. J Womens Health (Larchmt). 2019. PMID: 30508411 Free PMC article.
-
Sleep Fragmentation and Estradiol Suppression Decrease Fat Oxidation in Premenopausal Women.J Clin Endocrinol Metab. 2022 Jul 14;107(8):e3167-e3176. doi: 10.1210/clinem/dgac313. J Clin Endocrinol Metab. 2022. PMID: 35569055 Free PMC article.
-
Increased hypertension following hysterectomy among reproductive women in India.Am J Prev Cardiol. 2020 Nov 24;4:100131. doi: 10.1016/j.ajpc.2020.100131. eCollection 2020 Dec. Am J Prev Cardiol. 2020. PMID: 34327482 Free PMC article.
-
Menopause Is a Determinant of Breast Aromatase Expression and Its Associations With BMI, Inflammation, and Systemic Markers.J Clin Endocrinol Metab. 2017 May 1;102(5):1692-1701. doi: 10.1210/jc.2016-3606. J Clin Endocrinol Metab. 2017. PMID: 28323914 Free PMC article.
-
Gender-specific factors associated with hypertension among women of childbearing age: Findings from a nationwide survey in India.Front Cardiovasc Med. 2022 Dec 14;9:999567. doi: 10.3389/fcvm.2022.999567. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36588549 Free PMC article.
References
-
- Keshavarz H, Hillis SD, Kieke BA, Marchbanks PA. Hysterectomy surveillance. United States 1994–1999. MMWR CDC Surveill Summ. 2002;51:1–8. - PubMed
-
- Whiteman MK, Hillis SD, Jamieson DJ, Morrow B, Podgornik MN, Brett KM, et al. Inpatient hysterectomy surveillance in the United States, 2000–2004. Am J Obstet Gynecol. 2008 Jan;198(1):34. e1–7. - PubMed
-
- El-Hemaidi I, Gharaibeh A, Shehata H. Menorrhagia and bleeding disorders. Curr Opin Obstet Gynecol. 2007 Dec;19(6):513–20. - PubMed
-
- Spilsbury K, Semmens JB, Hammond I, Bolck A. Persistent high rates of hysterectomy in Western Australia: a population-based study of 83 000 procedures over 23 years. BJOG. 2006 Jul;113(7):804–9. - PubMed
Publication types
MeSH terms
Grants and funding
- AG012553/AG/NIA NIH HHS/United States
- T32 HL 007560/HL/NHLBI NIH HHS/United States
- AG012539/AG/NIA NIH HHS/United States
- AG012531/AG/NIA NIH HHS/United States
- U01 AG012495/AG/NIA NIH HHS/United States
- U01 AG012505/AG/NIA NIH HHS/United States
- AG012535/AG/NIA NIH HHS/United States
- AG012546/AG/NIA NIH HHS/United States
- NR004061/NR/NINR NIH HHS/United States
- U01 AG012554/AG/NIA NIH HHS/United States
- T32 HL007560/HL/NHLBI NIH HHS/United States
- AG012554/AG/NIA NIH HHS/United States
- U01 AG012535/AG/NIA NIH HHS/United States
- U01 AG012553/AG/NIA NIH HHS/United States
- U01 NR004061/NR/NINR NIH HHS/United States
- U01 AG012539/AG/NIA NIH HHS/United States
- AG012495/AG/NIA NIH HHS/United States
- U01 AG012546/AG/NIA NIH HHS/United States
- U01 AG012531/AG/NIA NIH HHS/United States
- AG012505/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
