

Conditioning regimens for allotransplants for diffuse large B-cell lymphoma: myeloablative or reduced intensity?
- PMID: 23007405
- PMCID: PMC3501720
- DOI: 10.1182/blood-2012-06-436725
Conditioning regimens for allotransplants for diffuse large B-cell lymphoma: myeloablative or reduced intensity?
Abstract
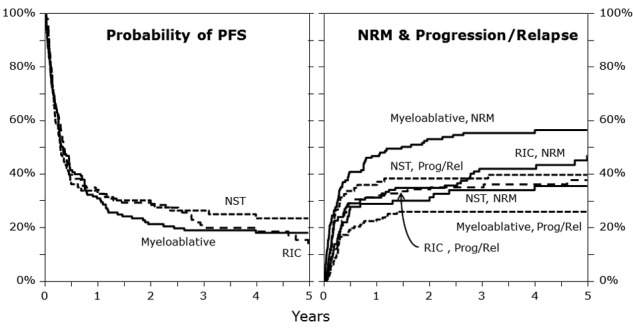
The best conditioning regimen before allogeneic transplantation for high-risk diffuse large B-cell lymphoma (DLBCL) remains to be clarified. We analyzed data from 396 recipients of allotransplants for DLBCL receiving myeloablative (MAC; n = 165), reduced intensity (RIC; n = 143), or nonmyeloablative conditioning (NMAC; n = 88) regimens. Acute and chronic GVHD rates were similar across the groups. Five-year nonrelapse mortality (NRM) was higher in MAC than RIC and NMAC (56% vs 47% vs 36%; P = .007). Five-year relapse/progression was lower in MAC than in RIC/NMAC (26% vs 38% vs 40%; P = .031). Five-year progression-free survival (15%-25%) and overall survival (18%-26%) did not differ significantly between the cohorts. In multivariate analysis, NMAC and more recent transplant year were associated with lower NRM, whereas a lower Karnofsky performance score (< 90), prior relapse resistant to therapy, and use of unrelated donors were associated with higher NRM. NMAC transplants, no prior use of rituximab, and prior relapse resistant to therapy were associated with a greater risk of relapse/progression. In conclusion, allotransplantation with RIC or NMAC induces long-term progression-free survival in selected DLBCL patients with a lower risk of NRM but with higher risk of lymphoma progression or relapse.
Figures
References
-
- Coiffier B, Lepage E, Briere J, et al. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med. 2002;346(4):235–242. - PubMed
-
- Sehn LH, Donaldson J, Chhanabhai M, et al. Introduction of combined CHOP plus rituximab therapy dramatically improved outcome of diffuse large B-cell lymphoma in British Columbia. J Clin Oncol. 2005;23(22):5027–5033. - PubMed
-
- Philip T, Guglielmi C, Hagenbeek A, et al. Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-Hodgkin's lymphoma. N Engl J Med. 1995;333(23):1540–1545. - PubMed
-
- van Kampen RJ, Canals C, Schouten HC, et al. Allogeneic stem-cell transplantation as salvage therapy for patients with diffuse large B-cell non-Hodgkin's lymphoma relapsing after an autologous stem-cell transplantation: an analysis of the European Group for Blood and Marrow Transplantation Registry. J Clin Oncol. 2011;29(10):1342–1348. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
