

Can a less radical surgery using photodynamic therapy with acridine orange be equal to a wide-margin resection?
- PMID: 23008027
- PMCID: PMC3563805
- DOI: 10.1007/s11999-012-2616-9
Can a less radical surgery using photodynamic therapy with acridine orange be equal to a wide-margin resection?
Abstract
Background: Wide-margin resections are an accepted method for treating soft tissue sarcoma. However, a wide-margin resection sometimes impairs function because of the lack of normal tissue. To preserve the normal tissue surrounding a tumor, we developed a less radical (ie, without a wide margin) surgical procedure using adjunctive photodynamic therapy and acridine orange for treating soft tissue sarcoma. However, whether this less radical surgical approach increases or decreases survival or whether it increases the risk of local recurrence remains uncertain.
Questions/purposes: We determined the survival, local recurrence, and limb function outcomes in patients treated with a less radical approach and adjunctive acridine orange therapy compared with those who underwent a conventional wide-margin resection.
Methods: We treated 170 patients with high-grade soft tissue sarcoma between 1999 and 2009. Fifty-one of these patients underwent acridine orange therapy. The remaining 119 patients underwent a conventional wide-margin resection for limb salvage surgery. We recorded the survival, local recurrence, and functional score (International Society of Limb Salvage [ISOLS]) score) for all the patients.
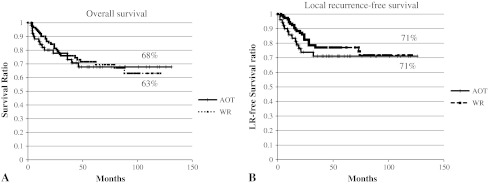
Results: The 10-year overall survival rates in the acridine orange therapy group and the conventional surgery group were 68% and 63%, respectively. The 10-year local recurrence rate was 29% for each group. The 5-year local recurrence rates for Stages II, III, and IV were 8%, 36%, and 40%, respectively, for the acridine orange group and 13%, 27%, and 33%, respectively, for the conventional surgery group. The average ISOLS score was 93% for the acridine orange group and 83% for the conventional therapy group.
Conclusion: Acridine orange therapy has the potential to preserve limb function without increasing the rate of local recurrence. This therapy may be useful for eliminating tumor cells with minimal damage to the normal tissue in patients with soft tissue sarcoma.
Level of evidence: Level IV, therapeutic study. See Guidelines for Authors for a complete description of the levels of evidence.
Figures

References
-
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–213. doi: 10.1097/01.sla.0000133083.54934.ae. - DOI - PMC - PubMed
-
- Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L, Kaplan R, Lacombe D, Verweij J. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1) Eur J Cancer. 2009;45:228–247. doi: 10.1016/j.ejca.2008.10.026. - DOI - PubMed
-
- Enneking WF, Dunham W, Gebhardt MC, Malawar M, Pritchard DJ. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin Orthop Relat Res. 1993;286:241–246. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
