

Design of a prostate cancer patient navigation intervention for a Veterans Affairs hospital
- PMID: 23009152
- PMCID: PMC3517303
- DOI: 10.1186/1472-6963-12-340
Design of a prostate cancer patient navigation intervention for a Veterans Affairs hospital
Abstract
Background: Patient navigation programs have been launched nationwide in an attempt to reduce racial/ethnic and socio-demographic disparities in cancer care, but few have evaluated outcomes in the prostate cancer setting. The National Cancer Institute-funded Chicago Patient Navigation Research Program (C-PNRP) aims to implement and evaluate the efficacy of a patient navigation intervention for predominantly low-income minority patients with an abnormal prostate cancer screening test at a Veterans Affairs (VA) hospital in Chicago.
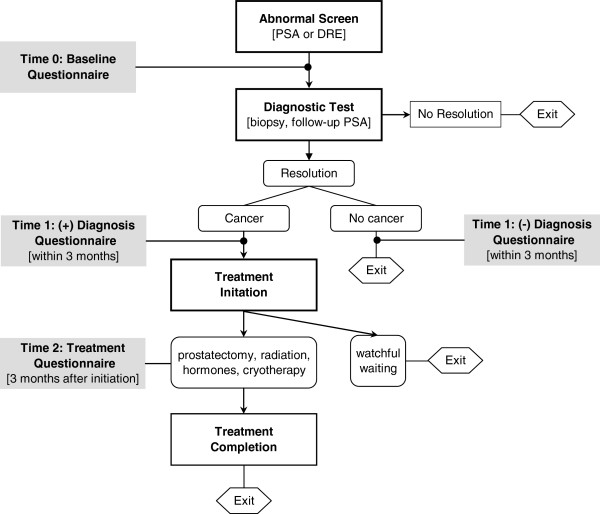
Methods/design: From 2006 through 2010, C-PNRP implemented a quasi-experimental intervention whereby trained social worker and lay health navigators worked with veterans with an abnormal prostate screen to proactively identify and resolve personal and systems barriers to care. Men were enrolled at a VA urology clinic and were selected to receive navigated versus usual care based on clinic day. Patient navigators performed activities to facilitate timely follow-up such as appointment reminders, transportation coordination, cancer education, scheduling assistance, and social support as needed. Primary outcome measures included time (days) from abnormal screening to diagnosis and time from diagnosis to treatment initiation. Secondary outcomes included psychosocial and demographic predictors of non-compliance and patient satisfaction. Dates of screening, follow-up visits, and treatment were obtained through chart audit, and questionnaires were administered at baseline, after diagnosis, and after treatment initiation. At the VA, 546 patients were enrolled in the study (245 in the navigated arm, 245 in the records-based control arm, and 56 in a subsample of surveyed control subjects).
Discussion: Given increasing concerns about balancing better health outcomes with lower costs, careful examination of interventions aimed at reducing healthcare disparities attain critical importance. While analysis of the C-PNRP data is underway, the design of this patient navigation intervention will inform other patient navigation programs addressing strategies to improve prostate cancer outcomes among vulnerable populations.
Figures
Similar articles
-
Navigating veterans with an abnormal prostate cancer screening test: a quasi-experimental study.BMC Health Serv Res. 2013 Aug 15;13:314. doi: 10.1186/1472-6963-13-314. BMC Health Serv Res. 2013. PMID: 23947435 Free PMC article. Clinical Trial.
-
Study protocol: a randomized controlled trial of patient navigation-activation to reduce cancer health disparities.BMC Cancer. 2010 Oct 13;10:551. doi: 10.1186/1471-2407-10-551. BMC Cancer. 2010. PMID: 20939928 Free PMC article. Clinical Trial.
-
Patient Navigation for Comprehensive Cancer Screening in High-Risk Patients Using a Population-Based Health Information Technology System: A Randomized Clinical Trial.JAMA Intern Med. 2016 Jul 1;176(7):930-7. doi: 10.1001/jamainternmed.2016.0841. JAMA Intern Med. 2016. PMID: 27273602 Clinical Trial.
-
State-of-the-science of patient navigation as a strategy for enhancing minority clinical trial accrual.Cancer. 2014 Apr 1;120 Suppl 7(0 7):1122-30. doi: 10.1002/cncr.28570. Cancer. 2014. PMID: 24643650 Free PMC article. Review.
-
Patient Navigation to Improve Cancer Screening in Underserved Populations: Reported Experiences, Opportunities, and Challenges.J Am Coll Radiol. 2018 Nov;15(11):1565-1572. doi: 10.1016/j.jacr.2018.03.001. Epub 2018 Apr 21. J Am Coll Radiol. 2018. PMID: 29685346 Review.
Cited by
-
Providers' Views on a Community-Wide Patient Navigation Program: Implications for Dissemination and Future Implementation.Health Promot Pract. 2016 May;17(3):382-90. doi: 10.1177/1524839916628865. Epub 2016 Mar 23. Health Promot Pract. 2016. PMID: 27009130 Free PMC article.
-
Factors Influencing the Implementation of Patient Navigation Programs for Adults with Complex Needs: A Scoping Review of the Literature.Health Serv Insights. 2021 Jul 17;14:11786329211033267. doi: 10.1177/11786329211033267. eCollection 2021. Health Serv Insights. 2021. PMID: 34349519 Free PMC article.
-
Examining care navigation: librarian participation in a team-based approach?J Med Libr Assoc. 2016 Apr;104(2):131-7. doi: 10.3163/1536-5050.104.2.007. J Med Libr Assoc. 2016. PMID: 27076800 Free PMC article.
-
The Independent Specialty Medical Advocate Model of Patient Navigation and Intermediate Health Outcomes in Newly Diagnosed Cancer Patients.J Oncol Navig Surviv. 2017 Oct;8(10):454-462. J Oncol Navig Surviv. 2017. PMID: 29796340 Free PMC article.
-
Navigation programs relevant for African American men with prostate cancer: a scoping review protocol.Syst Rev. 2022 Jun 14;11(1):122. doi: 10.1186/s13643-022-01993-6. Syst Rev. 2022. PMID: 35701771 Free PMC article.
References
-
- American Cancer Society. Cancer Facts & Figures 2011. Atlanta, GA: American Cancer Society; 2011.
-
- American Cancer Society. Facts & Figures for African Americans 2011. Atlanta, GA: American Cancer Society; 2011.
-
- Freeman HP, Muth BJ, Kerner JF. Expanding access to cancer screening and clinical follow-up among the medically underserved. Cancer Pract. 1995;3(1):19–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
