

Flexible bronchoscopy may decrease respiratory muscle strength: premedicational midazolam in focus
- PMID: 23009348
- PMCID: PMC3517408
- DOI: 10.1186/2049-6958-7-31
Flexible bronchoscopy may decrease respiratory muscle strength: premedicational midazolam in focus
Abstract
Background: Flexible bronchoscopy (FB) is a procedure accepted to be safe in general, with low complication rates reported. On the other hand, it is known that patients with pre-existing respiratory failure have developed hypoventilation following FB. In this study the effects of FB on respiratory muscle strength were investigated by measuring maximum respiratory pressures.
Methods: One hundred and forty patients, aged between 25 and 90 years, who had undergone diagnostic bronchoscopy between February 2012 and May 2012, were recruited to the study. Pre- and post-procedure maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP) were measured. A correlation between the MIP and MEP changes and patient characteristics and FB variables were investigated.
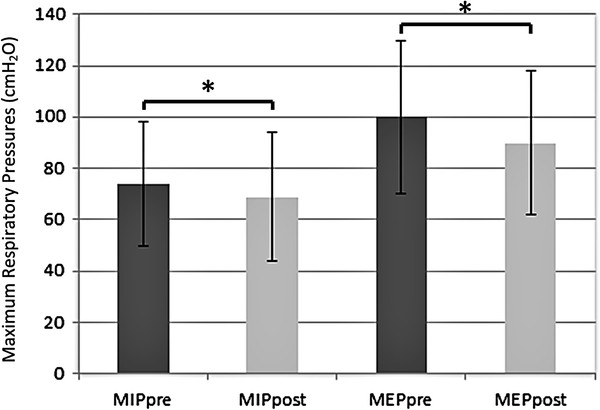
Results: Significant decreases in both MIP and MEP values were observed following FB (p < 0.001 for both). Decreases were attributed to the midazolam used for sedation. Significant decreases in respiratory muscle strengths were observed especially in the high-dose midazolam group, compared to both low-dose and non-midazolam groups.
Conclusions: It was determined that respiratory muscle weakness may arise post-procedure in patients who have undergone FB, and this is constitutively related to midazolam premedication. Respiratory muscle weakness might play a role in potential hypoventilation in critical patients who undergo FB.
Figures
Similar articles
-
Sedation during flexible bronchoscopy in patients with pre-existing respiratory failure: Midazolam versus Midazolam plus Alfentanil.Respiration. 2010;79(4):307-14. doi: 10.1159/000267227. Epub 2009 Dec 14. Respiration. 2010. PMID: 20016132
-
A Prospective Analysis of the Efficacy and Complications Associated With Deep Sedation With Midazolam During Fiberoptic Bronchoscopy.J Bronchology Interv Pulmonol. 2016 Apr;23(2):106-11. doi: 10.1097/LBR.0000000000000261. J Bronchology Interv Pulmonol. 2016. PMID: 27058712 Clinical Trial.
-
[A randomised study of midazolam for sedation in flexible bronchoscopy].Arch Bronconeumol. 2010 Jun;46(6):302-9. doi: 10.1016/j.arbres.2010.02.007. Epub 2010 Apr 13. Arch Bronconeumol. 2010. PMID: 20392554 Clinical Trial. Spanish.
-
Maximal Static Respiratory and Sniff Pressures in Healthy Children. A Systematic Review and Meta-Analysis.Ann Am Thorac Soc. 2019 Apr;16(4):478-487. doi: 10.1513/AnnalsATS.201808-506OC. Ann Am Thorac Soc. 2019. PMID: 30562038
-
The assessment of maximal respiratory mouth pressures in adults.Respir Care. 2009 Oct;54(10):1348-59. Respir Care. 2009. PMID: 19796415 Review.
Cited by
-
Intravenous Dexmedetomidine Provides Superior Patient Comfort and Tolerance Compared to Intravenous Midazolam in Patients Undergoing Flexible Bronchoscopy.Pulm Med. 2015;2015:727530. doi: 10.1155/2015/727530. Epub 2015 Oct 12. Pulm Med. 2015. PMID: 26543645 Free PMC article. Clinical Trial.
References
-
- Facciolongo N, Patelli M, Gasparini S, Lazzari Agli L, Salio M, Simonassi C, Del Prato B, Zanoni P. Incidence of complications in bronchoscopy. Multicentre prospective study of 20,986 bronchoscopies. Monaldi Arch Chest Dis. 2009;71(1):8–14. - PubMed
-
- Begin P, Grassino A. Inspiratory muscle dysfunction and chronic hypercapnia in chronic obstructive pulmonary disease. Am Rev Respir Dis. 1991;143(5 Pt 1):905–912. - PubMed
LinkOut - more resources
Full Text Sources
