

Cardiovascular disease risk in healthy children and its association with body mass index: systematic review and meta-analysis
- PMID: 23015032
- PMCID: PMC3458230
- DOI: 10.1136/bmj.e4759
Cardiovascular disease risk in healthy children and its association with body mass index: systematic review and meta-analysis
Abstract
Objectives: To describe the association and its magnitude between body mass index category, sex, and cardiovascular disease risk parameters in school aged children in highly developed countries.
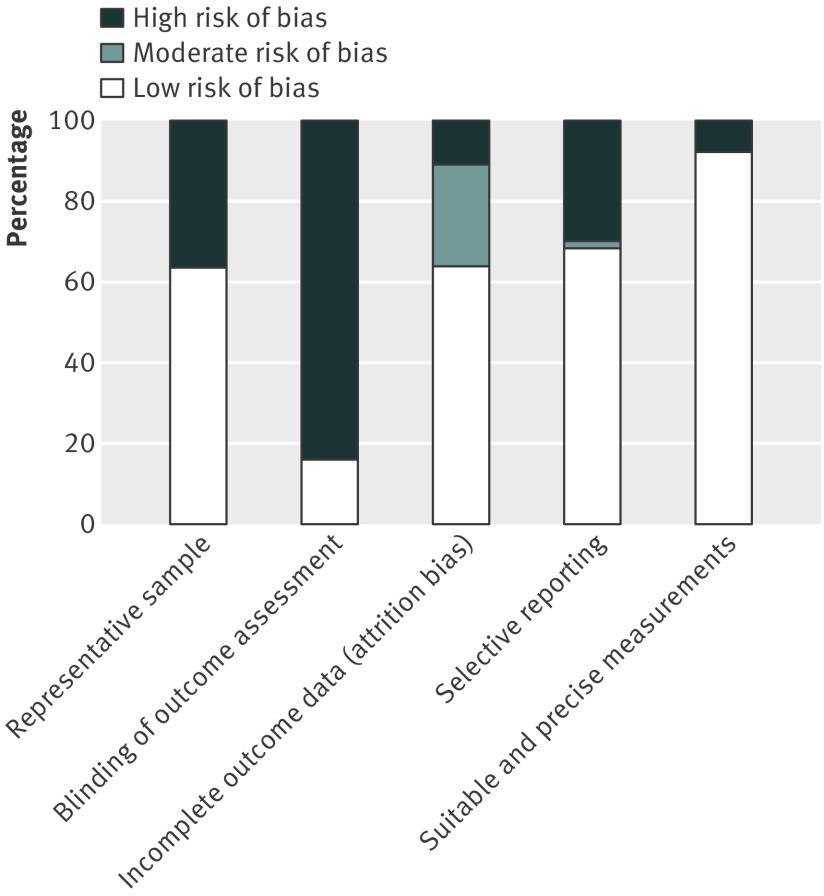
Design: Systematic review and meta-analysis. Quality of included studies assessed by an adapted version of the Cochrane Collaboration's risk of bias assessment tool. Results of included studies in meta-analysis were pooled and analysed by Review Manager version 5.1.
Data sources: Embase, PubMed, EBSCOHost's cumulative index to nursing and allied health literature, and the Web of Science databases for papers published between January 2000 and December 2011.
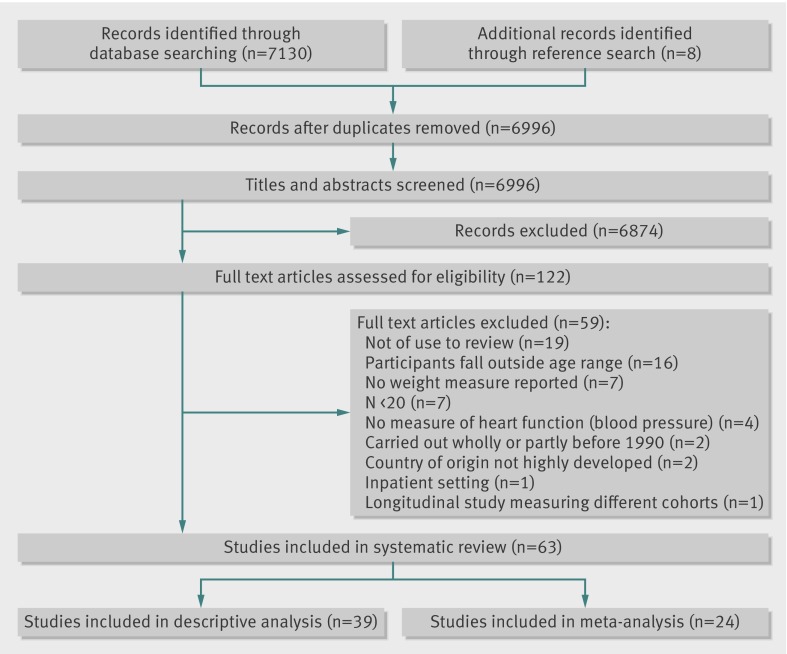
Review methods: Healthy children aged 5 to 15 in highly developed countries enrolled in studies done after 1990 and using prospective or retrospective cohort, cross sectional, case-control, or randomised clinical trial designs in school, outpatient, or community settings. Included studies had to report an objective measure of weight and at least one prespecified risk parameter for cardiovascular disease.
Results: We included 63 studies of 49 220 children. Studies reported a worsening of risk parameters for cardiovascular disease in overweight and obese participants. Compared with normal weight children, systolic blood pressure was higher by 4.54 mm Hg (99% confidence interval 2.44 to 6.64; n=12 169, eight studies) in overweight children, and by 7.49 mm Hg (3.36 to 11.62; n=8074, 15 studies) in obese children. We found similar associations between groups in diastolic and 24 h ambulatory systolic blood pressure. Obesity adversely affected concentrations of all blood lipids; total cholesterol and triglycerides were 0.15 mmol/L (0.04 to 0.25, n=5072) and 0.26 mmol/L (0.13 to 0.39, n=5138) higher in obese children, respectively. Fasting insulin and insulin resistance were significantly higher in obese participants but not in overweight participants. Obese children had a significant increase in left ventricular mass of 19.12 g (12.66 to 25.59, n=223), compared with normal weight children.
Conclusion: Having a body mass index outside the normal range significantly worsens risk parameters for cardiovascular disease in school aged children. This effect, already substantial in overweight children, increases in obesity and could be larger than previously thought. There is a need to establish whether acceptable parameter cut-off levels not considering weight are a valid measure of risk in modern children and whether methods used in their study and reporting should be standardised.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures

Comment in
-
Obesity in children and adolescents.BMJ. 2012 Sep 25;345:e5457. doi: 10.1136/bmj.e5457. BMJ. 2012. PMID: 23015033 No abstract available.
-
Don't rush into testing and treating children.BMJ. 2012 Oct 17;345:e6899. doi: 10.1136/bmj.e6899. BMJ. 2012. PMID: 23077356 No abstract available.
References
-
- World Health Organization. Obesity and overweight factsheet number 311. 2011. www.who.int/mediacentre/factsheets/fs311/en/index.html.
-
- Ebbeling CB, Pawlak DB, Ludwig DS. Childhood obesity: public-health crisis, common sense cure. Lancet 2002;360:473-82. - PubMed
-
- Flegal KM, Troiano RP. Changes in the distribution of body mass index of adults and children in the US population. Int J Obes 2000;24:807-18. - PubMed
-
- McPherson K, Marsh T, Brown M. Tackling obesities: future choices—modelling future trends in obesity and the impact on health: report for Foresight. Government Office for Science, 2007.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical