

The use of eccentrically biased resistance exercise to mitigate muscle impairments following anterior cruciate ligament reconstruction: a short review
- PMID: 23015852
- PMCID: PMC3445117
- DOI: 10.1177/1941738108327531
The use of eccentrically biased resistance exercise to mitigate muscle impairments following anterior cruciate ligament reconstruction: a short review
Abstract
Background: Novel interventions that can safely and effectively overload muscle early following anterior cruciate ligament reconstruction are needed to minimize atrophy and weakness that often becomes longstanding.
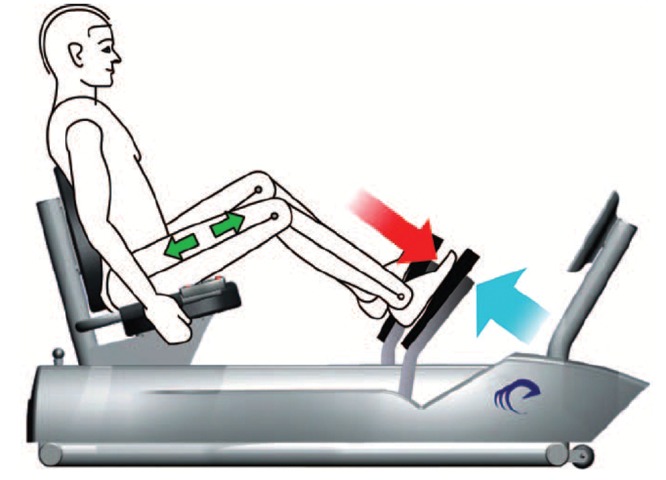
Evidence acquisition: Eccentrically induced forces can be safely applied during the early stages of rehabilitation following surgery and serve as a potent stimulus for increasing muscle size and strength.
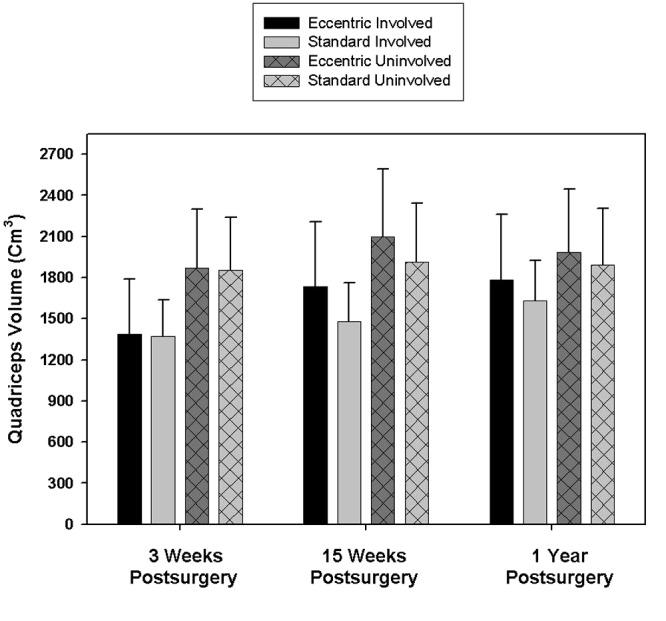
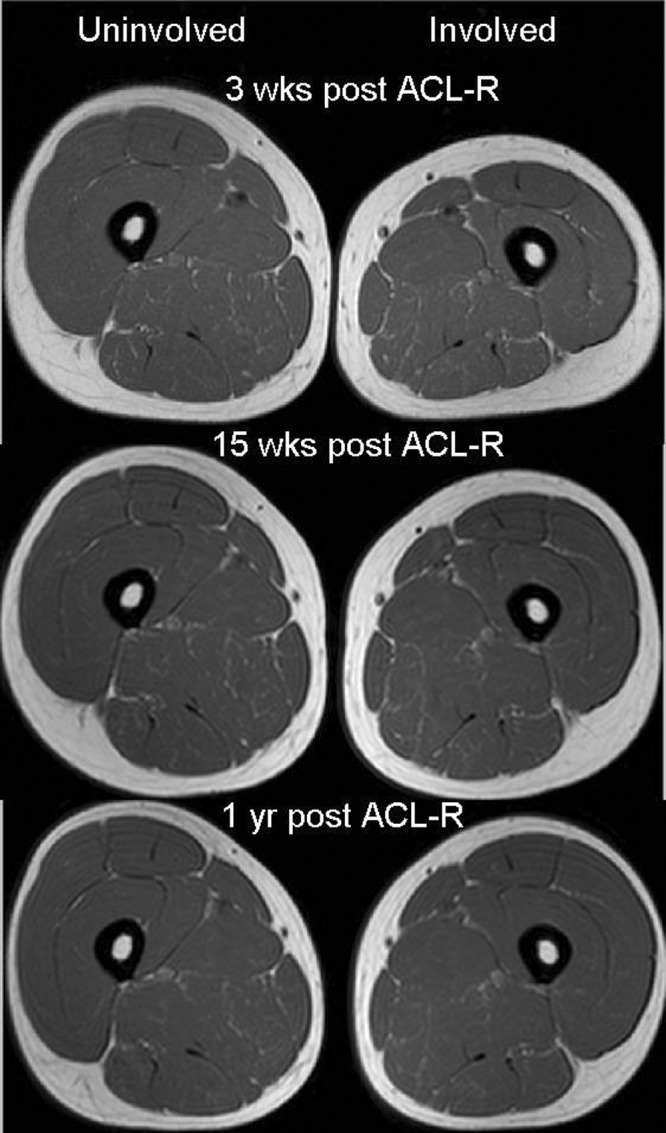
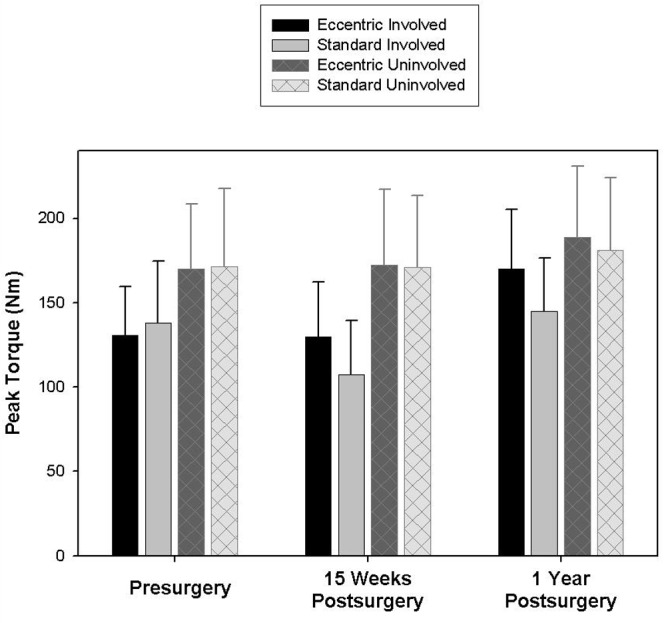
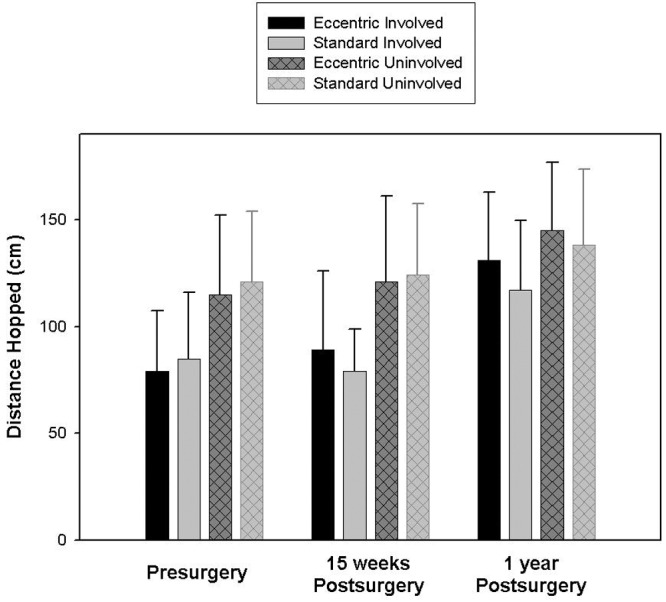
Results: Compared to a standard rehabilitation program, adding an early 12-week eccentric resistance-training program 3 weeks after anterior cruciate ligament reconstruction induces improvement in quadriceps and gluteus maximus volume at 15 weeks and at 1 year after surgery. Likewise, those who performed an eccentrically biased rehabilitation program also achieved greater improvements in quadriceps strength and hopping ability measured at 15 weeks and at 1 year after surgery.
Clinical relevance: There is potential to safely and feasibly perform eccentric contractions as part of a formal rehabilitation program following anterior cruciate ligament reconstruction.
Keywords: anterior cruciate ligament reconstruction; eccentric; outcomes; rehabilitation.
Conflict of interest statement
No potential conflict of interest declared.
Figures
References
-
- Anderson JL, Lamb SE, Barker KL, Davies S, Dodd CA, Beard DJ. Changes in muscle torque following anterior cruciate ligament reconstruction: a comparison between hamstrings and patella tendon graft procedures on 45 patients. Acta Orthop Scand. 2002;73(5):546-552 - PubMed
-
- Arangio GA, Chen C, Kalady M, Reed JF., 3rd Thigh muscle size and strength after anterior cruciate ligament reconstruction and rehabilitation. J Orthop Sports Phys Ther. 1997;26(5):238-243 - PubMed
-
- Elmqvist LG, Lorentzon R, Johansson C, Langstrom M, Fagerlund M, Fugl-Meyer AR. Knee extensor muscle function before and after reconstruction of anterior cruciate ligament tear. Scand J Rehabil Med. 1989;21(3):131-139 - PubMed
-
- Feller JA, Webster KE. A randomized comparison of patellar tendon and hamstring tendon anterior cruciate ligament reconstruction. Am J Sports Med. 2003;31(4):564-573 - PubMed
-
- Gerber JP, Marcus RL, Dibble LE, Greis PE, Burks RT, LaStayo PC. Effects of early progressive eccentric exercise on muscle structure after anterior cruciate ligament reconstruction. J Bone Joint Surg Am. 2007;89(3):559-570 - PubMed
LinkOut - more resources
Full Text Sources
