

Clinical management of scapulothoracic bursitis and the snapping scapula
- PMID: 23015932
- PMCID: PMC3445084
- DOI: 10.1177/1941738109338359
Clinical management of scapulothoracic bursitis and the snapping scapula
Abstract
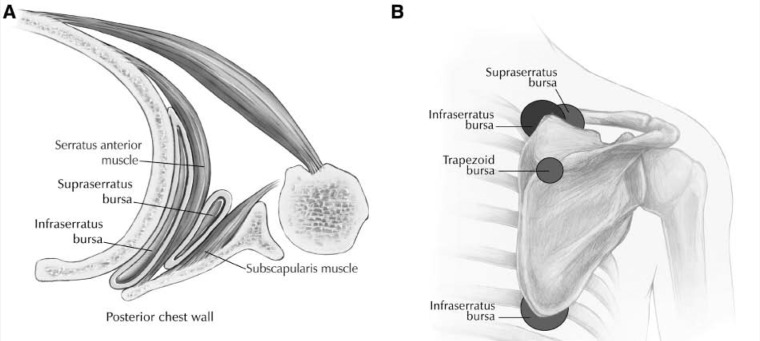
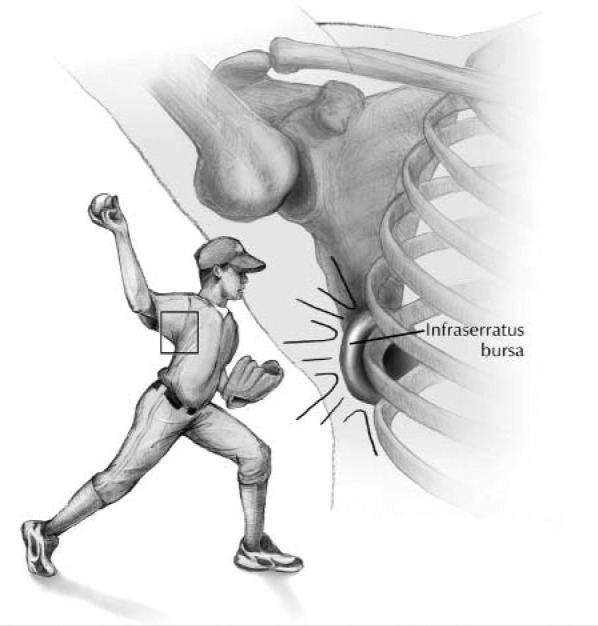
Context: Symptomatic scapulothoracic bursitis and crepitus are disorders of the scapulothoracic articulation that are often poorly understood. They can be a source of persistent pain and dysfunction in the active overhead throwing athlete. It is important to distinguish between scapulothoracic bursitis and scapulothoracic crepitus. Scapulothoracic bursitis refers to inflammation of the bursae secondary to trauma or overuse owing to sports activities or work. Scapulothoracic crepitus is defined by a grinding, popping, or thumping sound or sensation secondary to abnormal scapulothoracic motion.
Evidence acquisition: This article presents the causes, diagnosis, and management of these shoulder conditions in a manner that is relevant to clinicians, athletic trainers, and physical therapists, and it reviews relevant studies to determine the consensus on nonoperative treatment, as well as open and arthroscopic surgical treatment.
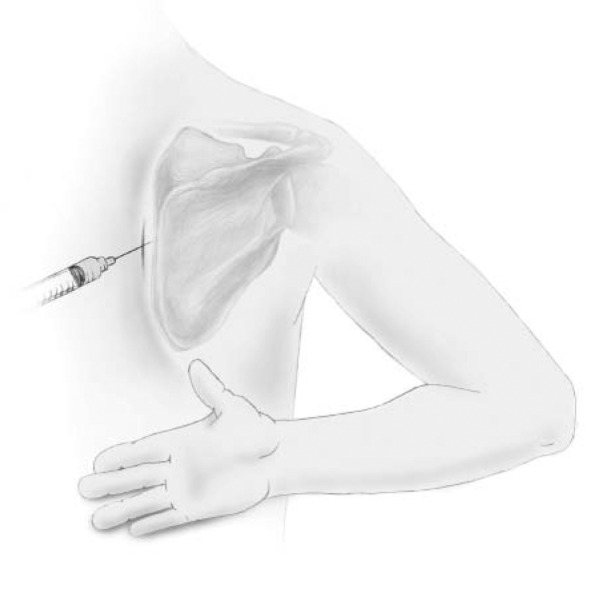
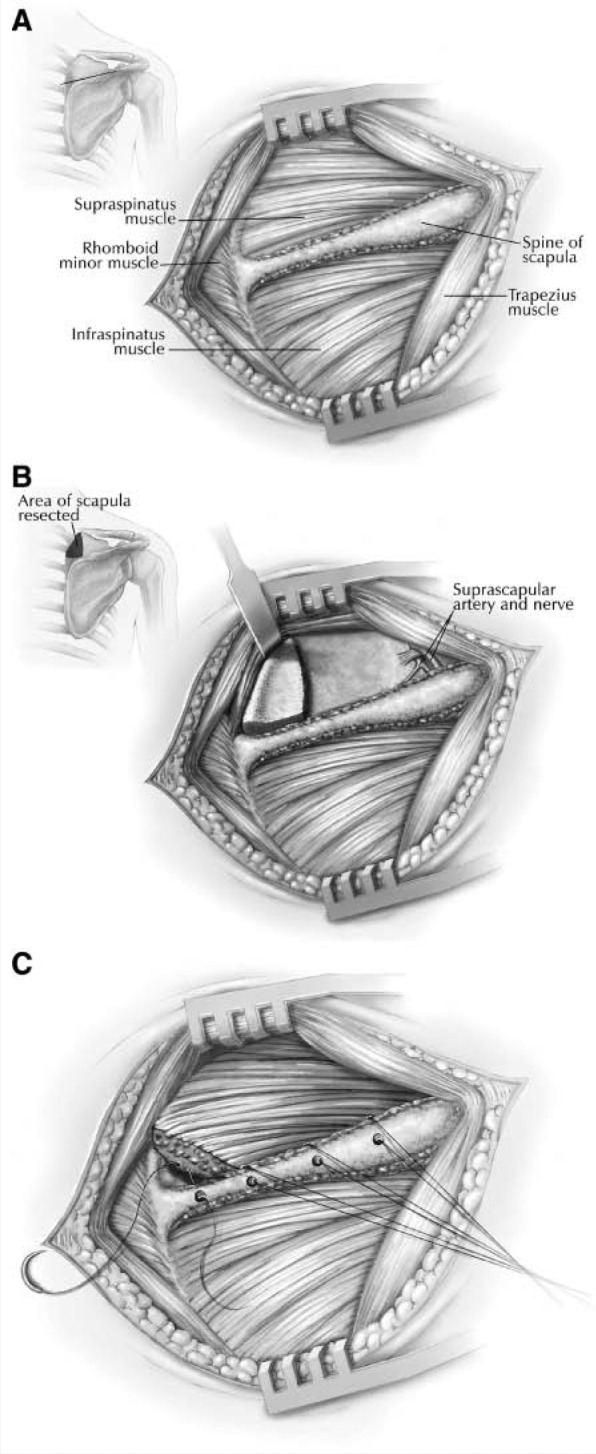
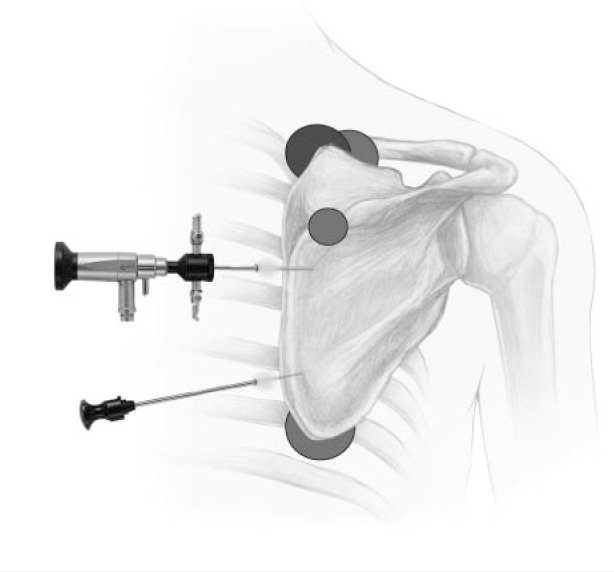
Results: The causes of scapulothoracic bursitis and crepitus include direct or indirect trauma, overuse syndromes, glenohumeral joint dysfunction, osseous abnormalities, muscle atrophy or fibrosis, and idiopathic causes. Scapulothoracic bursitis and crepitus remain primarily clinical diagnoses; however, imaging studies or local injections may also be helpful. The initial treatment of scapulothoracic bursitis and scapulothoracic crepitus should be nonoperative. Surgical treatment options include partial scapulectomy or resection of the superomedial angle of the scapula, open bursal resection, and arthroscopic bursectomy. Despite the lack of agreement among orthopaedic surgeons concerning which procedure is best for treating symptomatic scapulothoracic bursitis and crepitus, most reports have demonstrated good to excellent outcomes in a significantly high percentage of patients.
Conclusion: Clearly, the best initial approach to these conditions is a nonoperative treatment plan that combines scapular strengthening, postural reeducation, and core strength endurance. The addition of local modalities, nonsteroidal anti- inflammatory drugs, and localized injections may also be helpful. If an appropriate trial of nonoperative management proves unsuccessful, surgical correction can produce good results.
Keywords: scapulothoracic bursitis; shoulder; snapping scapula.
Conflict of interest statement
No potential conflict of interest declared.
Figures

References
-
- Arntz CT, Matsen FA. Partial scapulectomy for disabling scapulo-thoracic snapping. Orthop Trans. 1990;14:252-253
-
- Bateman JE. The Shoulder and Neck. 2nd ed. Philadelphia, PA: WB Saunders; 1978:185-194
-
- Bell SN, van Riet RP. Safe zone for arthroscopic resection of the superomedial scapular border in the treatment of snapping scapula syndrome. J Shoulder Elbow Surg. 2008;17:647-649 - PubMed
-
- Bergmann G. Biomechanics and pathomechanics of the shoulder joint with reference to prosthetic joint replacement. In: Kolbel R, Helbig B, Blauth W, eds. Shoulder Replacement. Berlin: Springer-Verlag; 1987:33-43
-
- Boinet W. Bulletin de la Societe Imperiale de Chirurgie dr Paris. 2nd ser. 1867;8:458
LinkOut - more resources
Full Text Sources
