

doi: 10.1177/1941738109347976.
Orthopaedic magnetic resonance imaging challenge: apophyseal avulsions at the pelvis
Affiliations
- PMID: 23015945
- PMCID: PMC3445104
- DOI: 10.1177/1941738109347976
Item in Clipboard
Orthopaedic magnetic resonance imaging challenge: apophyseal avulsions at the pelvis
Sports Health.
2010 May.
Abstract
Apophyseal avulsion injuries of the hip and pelvis are frequent athletic injuries in children and adolescents, most commonly associated with explosive movement or sprinting. This article details typically encountered apophyseal injuries and their appearance on magnetic resonance imaging.
Keywords: adolescent; apophyseal avulsion; hip and pelvis; magnetic resonance imaging.
Conflict of interest statement
No potential conflict of interest declared.
Figures

A frontal radiograph of the left hip shows subtle cortical irregularity of the anterior superior iliac spine (arrow).
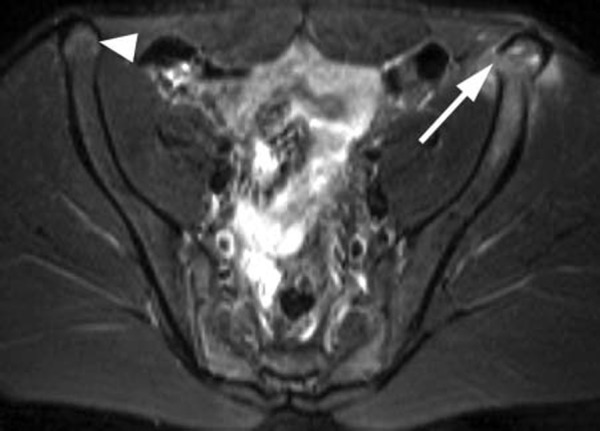
A mildly displaced fracture (arrow) is seen through the physis of the left anterior superior iliac spine. The edema in the fractured apophysis, iliac wing, and adjacent soft tissues is relatively mild, which is indicative of a subacute injury. Hyperintense signal in the contralateral anterior superior iliac spine (arrowhead) represents growth cartilage in this skeletally immature individual.
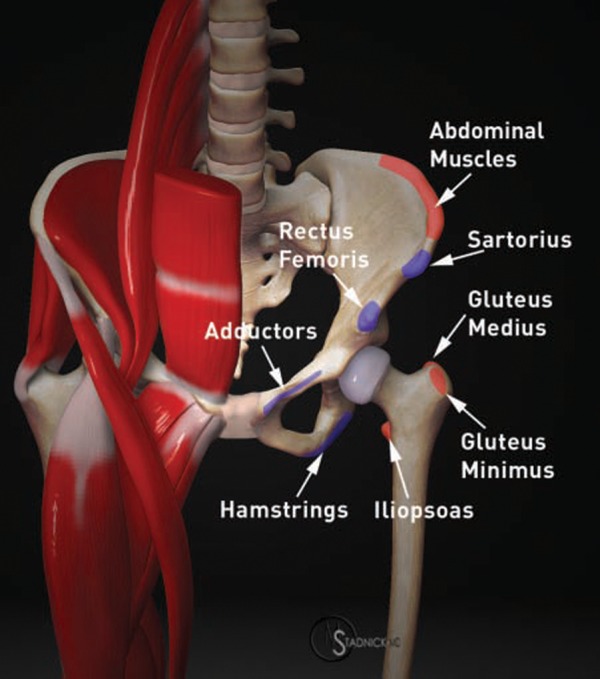
A 3-dimensional model of the pelvis illustrates the most common sites of apophyseal avulsion injury in adolescents, depicted in blue. Less common sites of apophyseal avulsion are indicated in red.

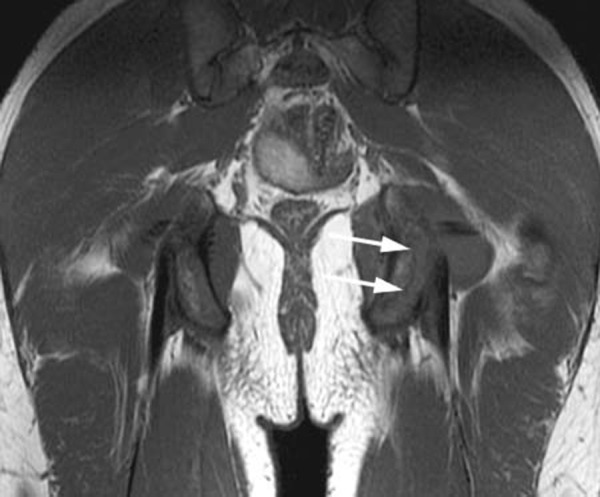
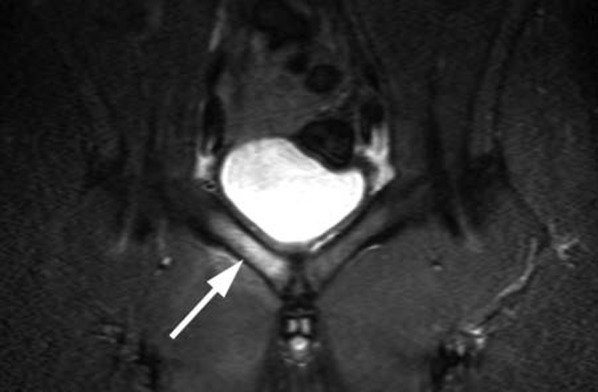
A coronal T1-weighted image through the posterior pelvis demonstrates a zone of intermediate signal (arrows) along the inferolateral aspect of the left ischial tuberosity in this 15-year-old football player complaining of left buttock pain.
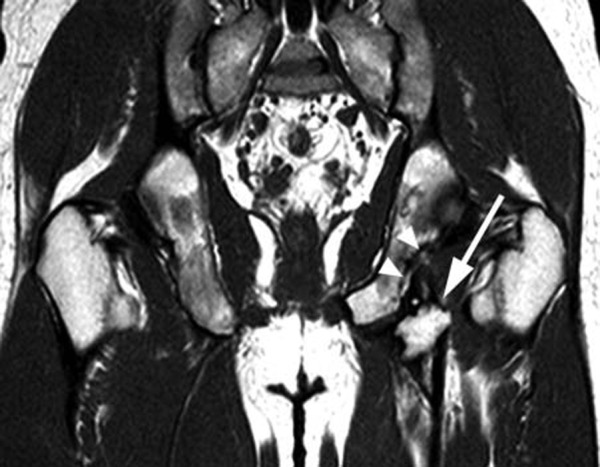
The corresponding coronal T2-weighted fat-suppressed image clearly depicts a fracture line (arrows) through the ischial tuberosity apophysis. An adjacent fluid collection most likely represents a distended bursa (arrowhead).
A coronal T1-weighted image of the pelvis demonstrates a displaced bony fragment (arrow) just distal to the left ischial tuberosity and a chronic-appearing defect of the ischium (arrowheads).

A 14-year-old male with avulsion of the left anterior inferior iliac spine. A T2-weighted coronal image reveals the avulsion of the apophysis at the direct head of the rectus femoris (arrow) with associated marrow and soft tissue edema (arrowheads). Note the normal anterior inferior iliac spine and rectus femoris tendon on the right (short arrow).

A sagittal fat-suppressed proton density–weighted image of the left hip (the same patient as Figure 7) depicts the avulsion injury involving both the direct (arrow) and the indirect (arrowhead) heads of the rectus femoris.

A 15-year-old girl with bilateral iliac crest avulsion on a coronal STIR image. Marrow edema and cortical irregularity (arrows) are evident at both iliac crests.

Iliac crest apophyseal avulsion on the left (arrow), as shown on a plain radiograph (not the patient in Figure 9). Bone resorption is present in the adjacent anterior superior iliac spine (arrowhead), consistent with an additional anterior superior iliac spine avulsion. In a minority of cases, avulsion injuries are multiple at the time of presentation.
A STIR coronal image of the symphysis pubis in a 16-year-old male soccer player who was initially thought to have osteomyelitis. Diffuse signal abnormality in the right superior pubic ramus (arrow) is present.

Inferior contour irregularity and marrow signal abnormality are demonstrated (in the same patient as Figure 11) in the right parasymphyseal region (arrow) at the origin of the adductor longus, consistent with an avulsion injury.
References
-
- Bencardino JT, Mellado JM. Hamstring injuries of the hip. Magn Reson Imaging Clin N Am. 2005;13:677-690 - PubMed
-
- Boyd KT, Peirce NS, Batt ME. Common hip injuries in sports. Sports Med. 1997;24(4):273-288 - PubMed
-
- Combs J. Hip and pelvis avulsion injuries in adolescents. Phys Sportsmed. 1994;22:41-49 - PubMed
-
- Cunningham PM, Brennan D, O’Connell M, MacMahon P, O’Neill P, Eustace S. Patterns of bone and soft-tissue injury at the symphysis pubis in soccer players: observations at MRI. AJR Am J Roentgenol. 2007;188:W291-W296 - PubMed
-
- Diehl JJ, Best TM, Kaeding CC. Classification and return-to-play considerations for stress fractures. Clin Sports Med. 2006;25:17-28 - PubMed
LinkOut - more resources
Full Text Sources
