

Rehabilitation of Concussion and Post-concussion Syndrome
- PMID: 23016082
- PMCID: PMC3435903
- DOI: 10.1177/1941738111433673
Rehabilitation of Concussion and Post-concussion Syndrome
Abstract
Context: Prolonged symptoms after concussion are called post-concussion syndrome (PCS), which is a controversial disorder with a wide differential diagnosis.
Evidence acquisition: MEDLINE and PubMed searches were conducted for the years 1966 to 2011 using the search terms brain concussion/complications OR brain concussion/diagnosis OR brain concussion/therapy AND sports OR athletic injuries. Secondary search terms included post-concussion syndrome, trauma, symptoms, metabolic, sports medicine, cognitive behavioral therapy, treatment and rehabilitation. Additional articles were identified from the bibliographies of recent reviews.
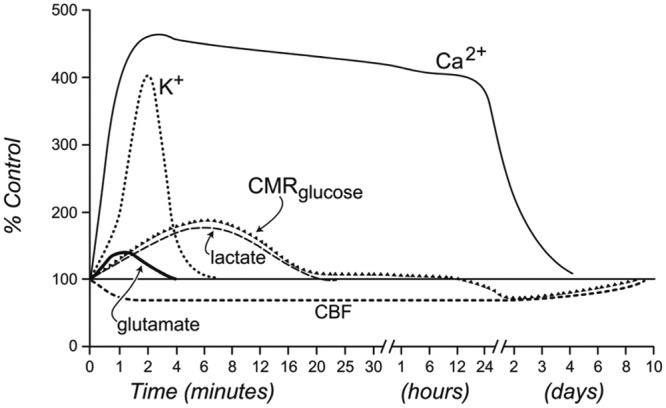
Results: Of 564 studies that fulfilled preliminary search criteria, 119 focused on the diagnosis, pathophysiology, and treatment/rehabilitation of concussion and PCS and formed the basis of this review. Rest is the primary treatment for the acute symptoms of concussion. Ongoing symptoms are either a prolonged version of the concussion pathophysiology or a manifestation of other processes, such as cervical injury, migraine headaches, depression, chronic pain, vestibular dysfunction, visual dysfunction, or some combination of conditions. The pathophysiology of ongoing symptoms from the original concussion injury may reflect multiple causes: anatomic, neurometabolic, and physiologic.
Conclusions: Treatment approaches depend on the clinician's ability to differentiate among the various conditions associated with PCS. Early education, cognitive behavioral therapy, and aerobic exercise therapy have shown efficacy in certain patients but have limitations of study design. An algorithm is presented to aid clinicians in the evaluation and treatment of concussion and PCS and in the return-to-activity decision.
Keywords: cognitive behavioral therapy; concussion; physiology; post-concussion syndrome; rehabilitation.
Figures

References
-
- Agrawal D, Gowda NK, Bal CS, Pant M, Mahapatra AK. Is medial temporal injury responsible for pediatric postconcussion syndrome? A prospective controlled study with single-photon emission computerized tomography. J Neurosurg. 2005;102(2)(suppl):167-171 - PubMed
-
- Al Sayegh A, Sandford D, Carson AJ. Psychological approaches to treatment of postconcussion syndrome: a systematic review. J Neurol Neurosurg Psychiatry. 2010;81(10):1128-1134 - PubMed
-
- Alsalaheen BA, Mucha A, Morris LO, et al. Vestibular rehabilitation for dizziness and balance disorders after concussion. J Neurol Phys Ther. 2010;34(2):87-93 - PubMed
-
- Arciniegas DB, Topkoff JL. Applications of the P50 evoked response to the evaluation of cognitive impairments after traumatic brain injury. Phys Med Rehabil Clin N Am. 2004;15(1):177-203 - PubMed
-
- Baldwin SA, Fugaccia I, Brown DR, Brown LV, Scheff SW. Blood-brain barrier breach following cortical contusion in the rat. J Neurosurg. 1996;85(3):476-481 - PubMed
LinkOut - more resources
Full Text Sources
Medical
