

Tendinopathy in sport
- PMID: 23016086
- PMCID: PMC3435934
- DOI: 10.1177/1941738112440957
Tendinopathy in sport
Abstract
Context: Tendinopathy is increasing in prevalence and accounts for a substantial part of all sports injuries and occupational disorders. Despite the magnitude of the disorder, high-quality scientific data on etiology and available treatments have been limited.
Evidence acquisition: The authors conducted a MEDLINE search on tendinopathy, or "tendonitis" or "tendinosis" or "epicondylitis" or "jumpers knee" from 1980 to 2011. The emphasis was placed on updates on epidemiology, etiology, and recent patient-oriented Level 1 literature.
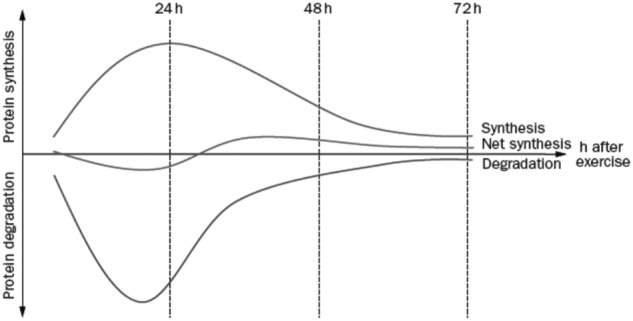
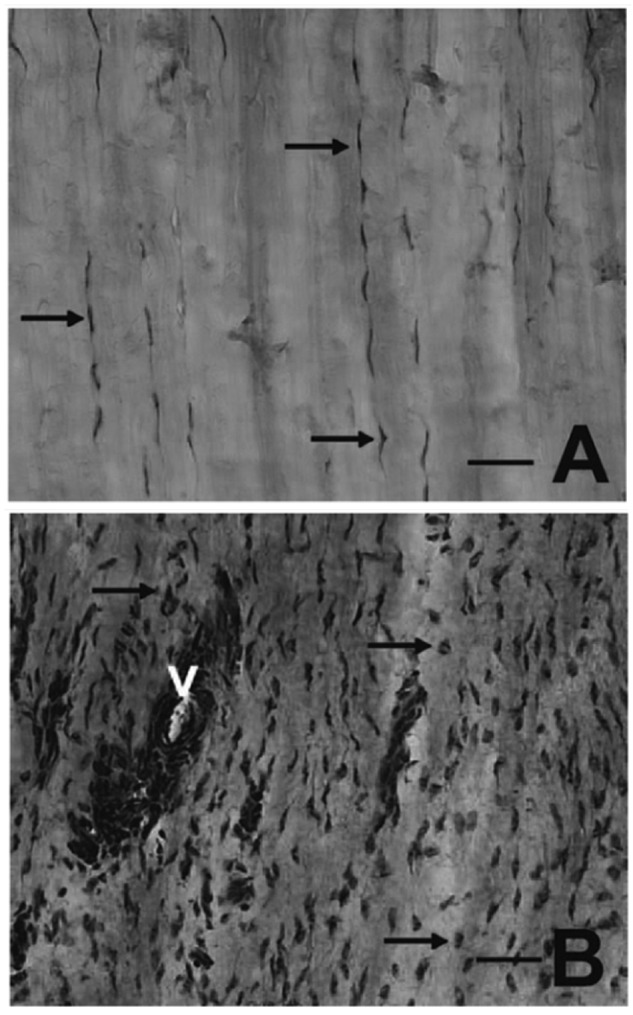
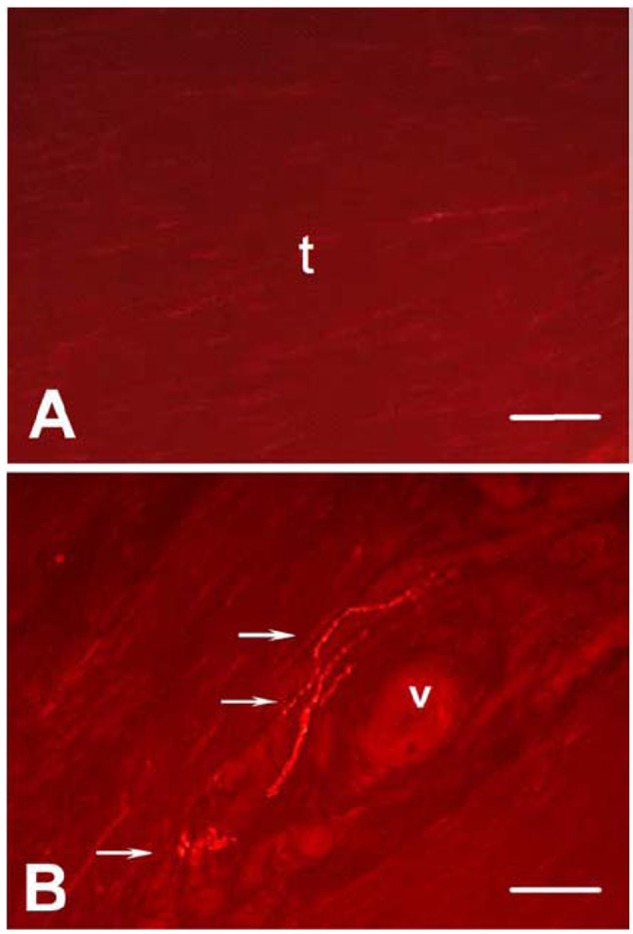
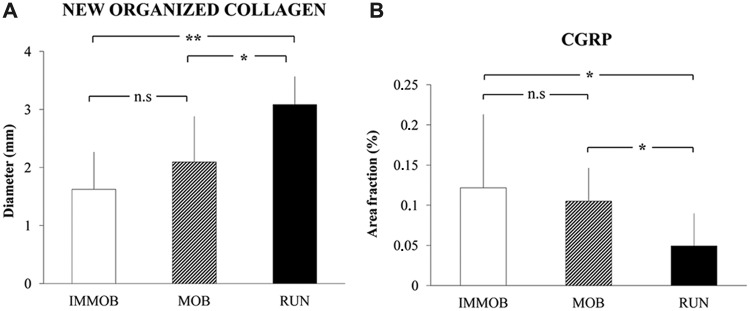
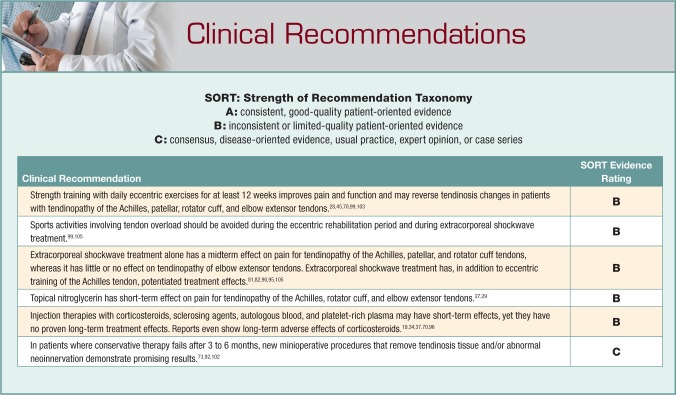
Results: Repetitive exposure in combination with recently discovered intrinsic factors, such as genetic variants of matrix proteins, and metabolic disorders is a risk factor for the development of tendinopathy. Recent findings demonstrate that tendinosis is characterized by a fibrotic, failed healing response associated with pathological vessel and sensory nerve ingrowth. This aberrant sensory nerve sprouting may partly explain increased pain signaling and partly, by release of neuronal mediators, contribute to the fibrotic alterations observed in tendinopathy. The initial nonoperative treatment should involve eccentric exercise, which should be the cornerstone (basis) of treatment of tendinopathy. Eccentric training combined with extracorporeal shockwave treatment has in some reports shown higher success rates compared to any therapies alone. Injection therapies (cortisone, sclerosing agents, blood products including platelet-rich plasma) may have short-term effects but have no proven long-term treatment effects or meta-analyses to support them. For epicondylitis, cortisone injections have demonstrated poorer long-time results than conservative physiotherapy. Today surgery is less indicated because of successful conservative therapies. New minioperative procedures that, via the endoscope, remove pathologic tissue or abnormal neoinnervation demonstrate promising results but need confirmation by Level 1 studies.
Conclusions: Novel targeted therapies are emerging, but multicenter trials are needed to confirm the results of exercise and mini-invasive treatments.
Keywords: pain; tendinopathy; tendinosis; tendon.
Figures

References
-
- Ackermann PW, Li J, Lundeberg T, Kreicbergs A. Neuronal plasticity in relation to nociception and healing of rat achilles tendon. J Orthop Res. 2003;21(3):432-441 - PubMed
-
- Ackermann PW, Salo PT, Hart DA. Neuronal pathways in tendon healing. Front Biosci. 2009;14:5165-5187 - PubMed
-
- Alfredson H. Ultrasound and Doppler-guided mini-surgery to treat midportion Achilles tendinosis: results of a large material and a randomised study comparing two scraping techniques. Br J Sports Med. 2011;45(5):407-410 - PubMed
-
- Alfredson H, Forsgren S, Thorsen K, Fahlstrom M, Johansson H, Lorentzon R. Glutamate NMDAR1 receptors localised to nerves in human Achilles tendons: Implications for treatment? Knee Surg Sports Traumatol Arthrosc. 2001;9(2):123-126 - PubMed
LinkOut - more resources
Full Text Sources
Medical
