

The basic science of human knee menisci: structure, composition, and function
- PMID: 23016106
- PMCID: PMC3435920
- DOI: 10.1177/1941738111429419
The basic science of human knee menisci: structure, composition, and function
Abstract
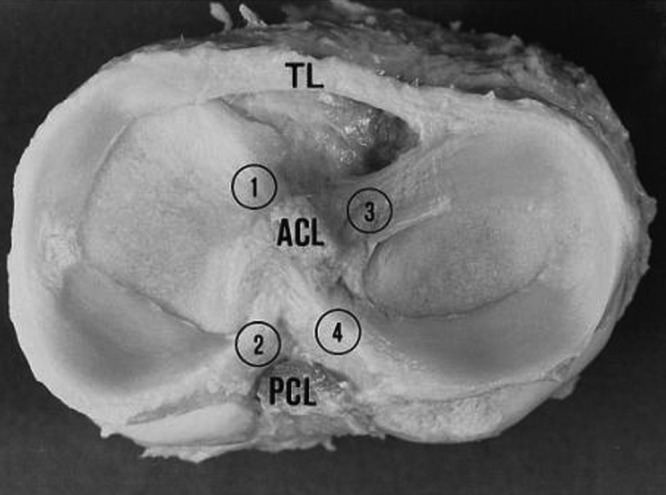
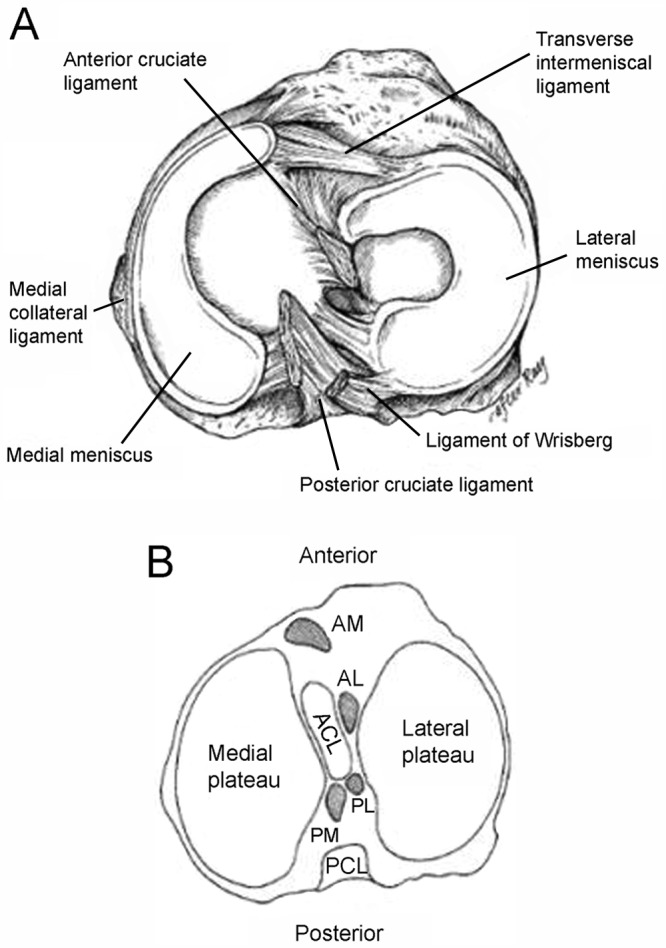
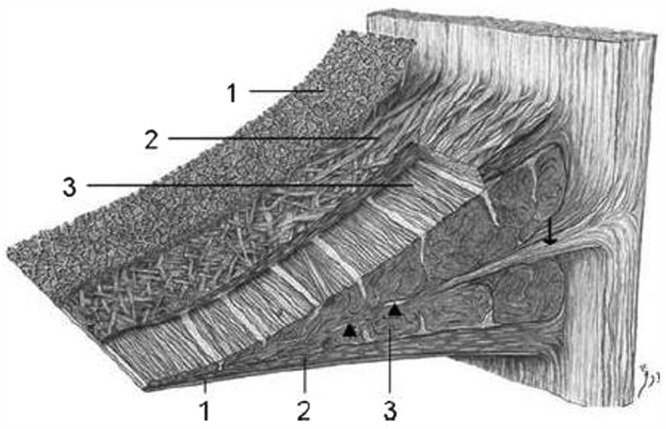
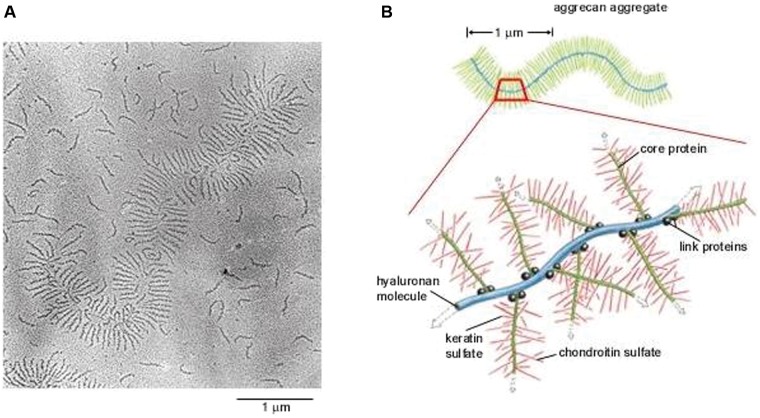
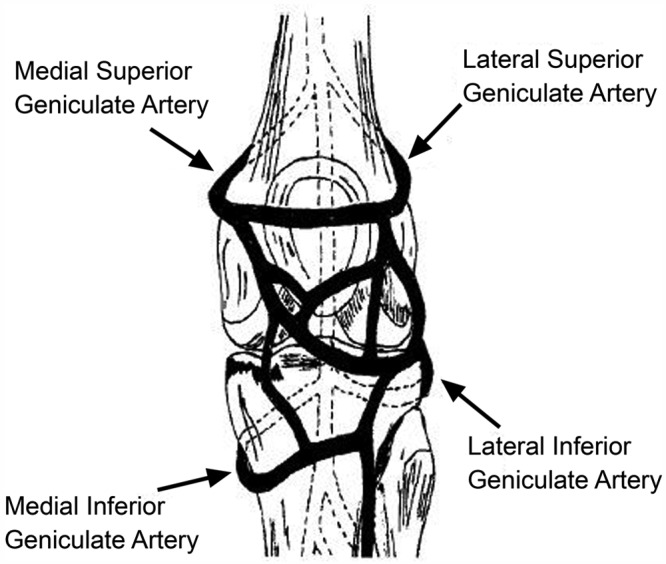
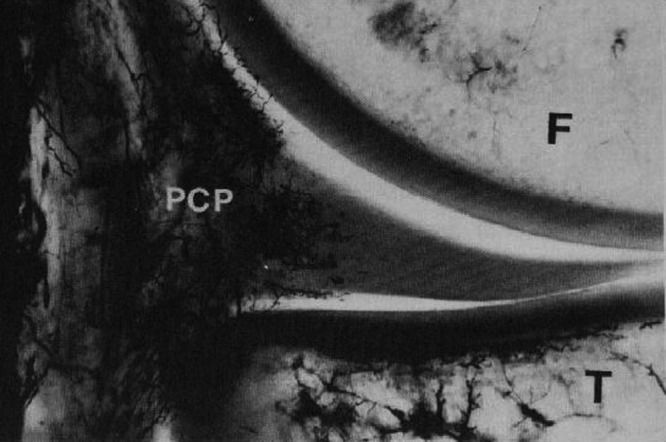
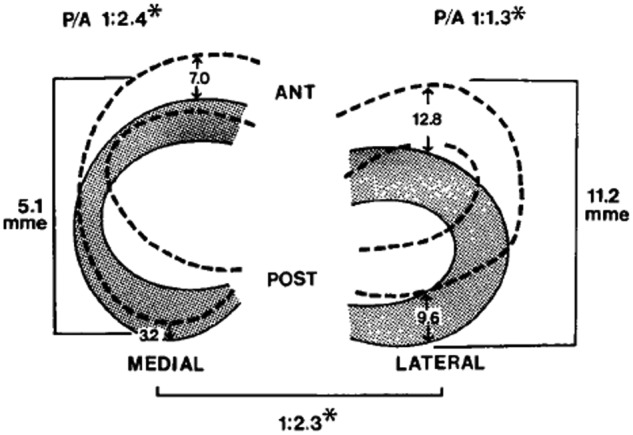
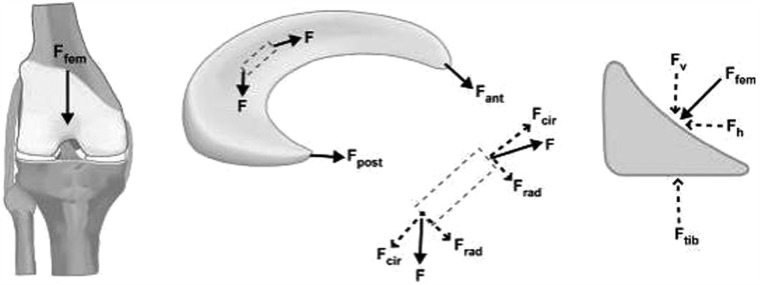
Context: Information regarding the structure, composition, and function of the knee menisci has been scattered across multiple sources and fields. This review contains a concise, detailed description of the knee menisci-including anatomy, etymology, phylogeny, ultrastructure and biochemistry, vascular anatomy and neuroanatomy, biomechanical function, maturation and aging, and imaging modalities.
Evidence acquisition: A literature search was performed by a review of PubMed and OVID articles published from 1858 to 2011.
Results: This study highlights the structural, compositional, and functional characteristics of the menisci, which may be relevant to clinical presentations, diagnosis, and surgical repairs.
Conclusions: An understanding of the normal anatomy and biomechanics of the menisci is a necessary prerequisite to understanding the pathogenesis of disorders involving the knee.
Figures

References
-
- Adams ME, Hukins DWL. The extracellular matrix of the meniscus. In: Mow VC, Arnoczky SP, Jackson DW. eds. Knee Meniscus: Basic and Clinical Foundations. New York, NY: Raven Press; 1992:15-282016
-
- Adams ME, McDevitt CA, Ho A, Muir H. Isolation and characterization of high-buoyant-density proteoglycans from semilunar menisci. J Bone Joint Surg Am. 1986;68:55-64 - PubMed
-
- Ahmed AM, Burke DL. In-vitro measurement of static pressure distribution in synovial joints: part I. Tibial surface of the knee. J Biomech Eng. 1983;185:290-294 - PubMed
-
- Akgun U, Kogaoglu B, Orhan EK, Baslo MB, Karahan M. Possible reflex pathway between medial meniscus and semi-membranous muscle: an experimental study in rabbits. Knee Surg Sports Traumatol Arthrosc. 2008;16(9):809-814 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
