

Mechanical thrombectomy in acute stroke: utilization variances and impact of procedural volume on inpatient mortality
- PMID: 23017430
- PMCID: PMC4085991
- DOI: 10.1016/j.jstrokecerebrovasdis.2012.08.007
Mechanical thrombectomy in acute stroke: utilization variances and impact of procedural volume on inpatient mortality
Abstract
Background: An increasing number of endovascular mechanical thrombectomy procedures are being performed for the treatment of acute ischemic stroke. This study examines variances in the allocation of these procedures in the United States at the hospital level. We investigate operative volume across centers performing mechanical revascularization and establish that procedural volume is independently associated with inpatient mortality.
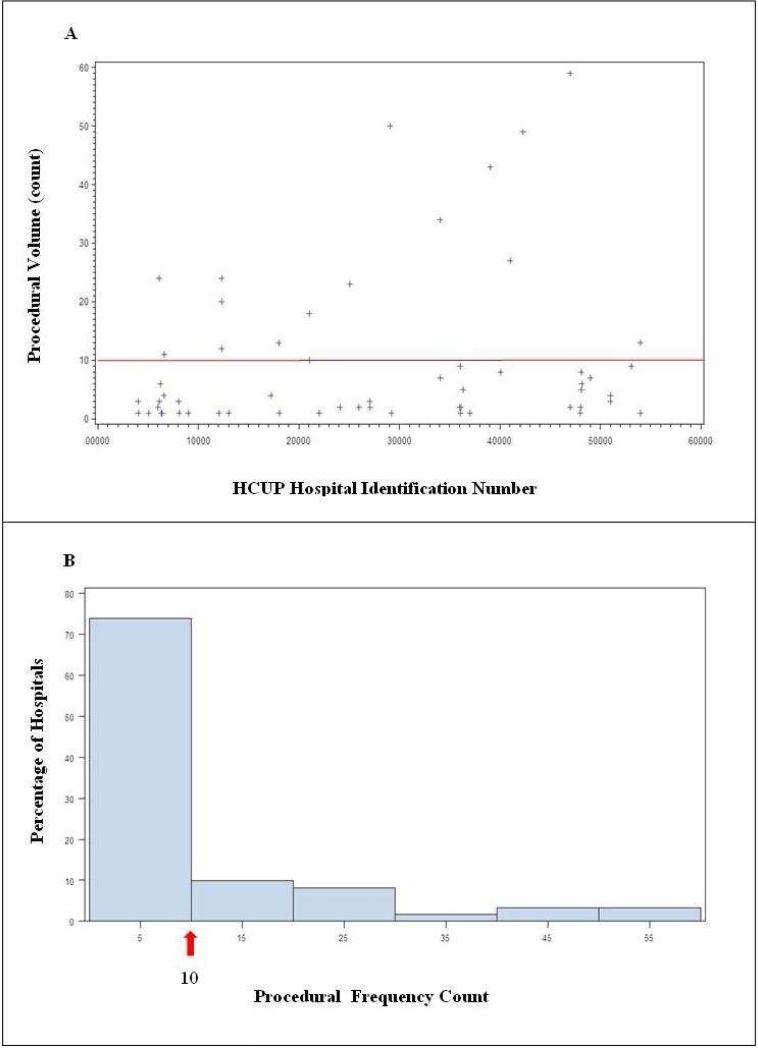
Methods: Data was collected using the Nationwide Inpatient Sample database in the United States for 2008. Medical centers performing mechanical thrombectomy were identified using International Classification of Diseases, 9th revision codes, and procedural volumes were evaluated according to hospital size, location, control/ownership, geographic characteristics, and teaching status. Inpatient mortality was compared for hospitals performing ≥10 mechanical thrombectomy procedures versus those performing<10 procedures annually. After univariate analysis identified the factors that were significantly related to mortality, multivariable logistic regression was performed to compare mortality outcome by hospital procedure volume independent of covariates.
Results: Significant allocation differences existed for mechanical thrombectomy procedures according to hospital size (P<.001), location (P<.0001), control/ownership (P<.0001), geography (P<.05), and teaching status (P<.0001). Substantial procedural volume was independently associated with decreased mortality (P=.0002; odds ratio 0.49) when adjusting for demographic covariates.
Conclusions: The number of mechanical thrombectomy procedures performed nationally remains relatively low, with a disproportionate distribution of neurointerventional centers in high-volume, urban teaching hospitals. Procedural volume is associated with mortality in facilities performing mechanical thrombectomy for acute ischemic stroke patients. These results suggest a potential benefit for treatment centralization to facilities with substantial operative volume.
Keywords: Acute stroke; mortality; neurointerventional procedures; thrombectomy.
Copyright © 2013 National Stroke Association. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Towfighi A, Saver JL. Stroke declines from third to fourth leading cause of death in the United States: historical perspective and challenges ahead. Stroke. 2011;42:2351–2355. - PubMed
-
- NINDS rt-PA Stroke Study Group Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333:1581–1587. - PubMed
-
- Del Zoppo GJ, Saver JL, Jauch EC, et al. American Heart Association Stroke Council. Expansion of the time window for treatment of acute ischemic stroke with intravenous tissue plasminogen activator: a science advisory from the American Heart Association/American Stroke Association. Stroke. 2009;40:2945–2948. - PMC - PubMed
-
- Rha JH, Saver JL. “The impact of recanalization on ischemic stroke outcome: a meta-analysis,”. Stroke. 2007;38:967–973. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
