

Cerebral β-amyloid deposition predicts HIV-associated neurocognitive disorders in APOE ε4 carriers
- PMID: 23018443
- PMCID: PMC3576852
- DOI: 10.1097/QAD.0b013e32835a117c
Cerebral β-amyloid deposition predicts HIV-associated neurocognitive disorders in APOE ε4 carriers
Abstract
Objective: The apolipoprotein E (APOE) ε4 allele enhances cerebral accumulation of β-amyloid (Aβ) and is a major risk factor for sporadic Alzheimer's disease. We hypothesized that HIV-associated neurocognitive disorders (HAND) would be associated with the APOE ε4 genotype and cerebral Aβ deposition.
Design: Clinicopathological study of HIV-infected adults from four prospective cohorts in the US National NeuroAIDS Tissue Consortium.
Methods: We used multivariable logistic regressions to model outcomes [Aβ plaques (immunohistochemistry) and HAND (standard criteria)] on predictors [APOE ε4 (allelic discrimination assay), older age (≥50 years), Aβ plaques, and their two-way interactions] and comorbid factors.
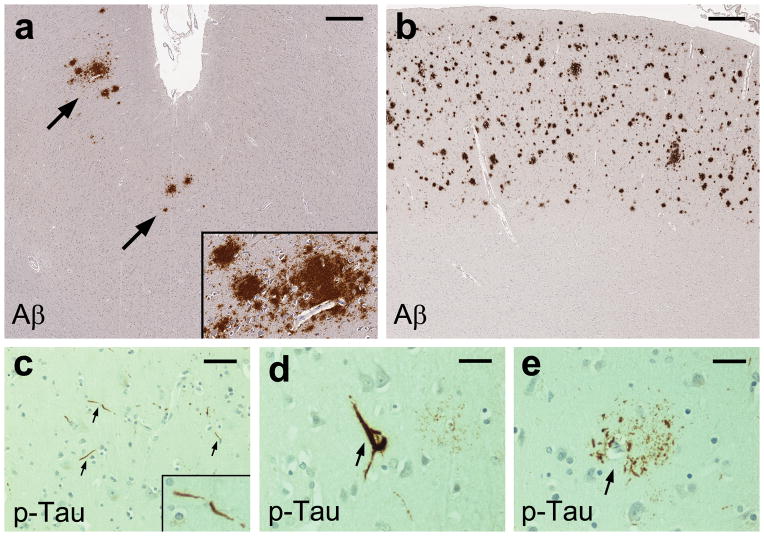
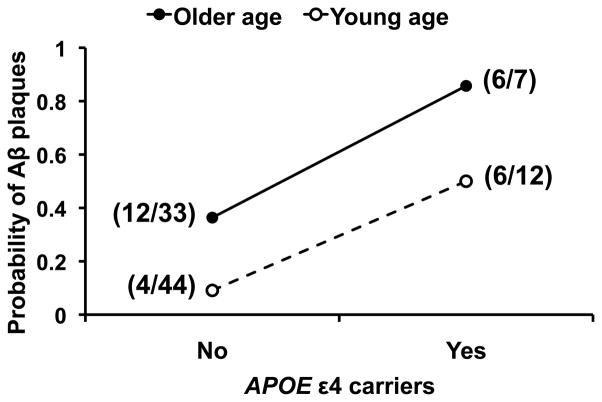
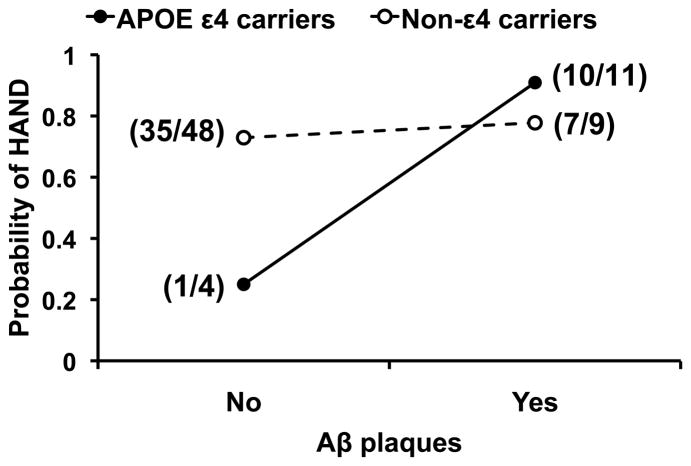
Results: Isocortical Aβ deposits generally occurred as diffuse plaques and mild-to-moderate amyloid angiopathy. Isocortical phospho-Tau-immunoreactive neurofibrillary lesions were sparse. The APOE ε4 and older age were independently associated with the presence of Aβ plaques [adjusted odds ratio (OR) 10.16 and 5.77, 95% confidence interval (CI) 2.89 - 35.76 and 1.91-17.48, P = 0.0003 and 0.0019, respectively, n = 96]. The probability of HAND was increased in the presence of Aβ plaques among APOE ε4 carriers (adjusted OR 30.00, 95% CI 1.41-638.63, P = 0.029, n = 15), but not in non-ε4 carriers (n = 57).
Conclusion: The APOE ε4 and older age increased the likelihood of cerebral Aβ plaque deposition in HIV-infected adults. Generally, Aβ plaques in HIV brains were immunohistologically different from those in symptomatic Alzheimer's disease brains. Nonetheless, Aβ plaques were associated with HAND among APOE ε4 carriers. The detection of APOE ε4 genotype and cerebral Aβ deposition biomarkers may be useful in identifying living HAND patients who could benefit from Aβ-targeted therapies.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
- U24 MH100931/MH/NIMH NIH HHS/United States
- R01 AG043384/AG/NIA NIH HHS/United States
- R24 NS045491/NS/NINDS NIH HHS/United States
- R25 MH081482/MH/NIMH NIH HHS/United States
- R24 MH059745/MH/NIMH NIH HHS/United States
- R24 NS038841/NS/NINDS NIH HHS/United States
- P50 AG016570/AG/NIA NIH HHS/United States
- U01 MH083501/MH/NIMH NIH HHS/United States
- U01 MH083506/MH/NIMH NIH HHS/United States
- U01 AI035040/AI/NIAID NIH HHS/United States
- U24 MH100929/MH/NIMH NIH HHS/United States
- U01 MH083507/MH/NIMH NIH HHS/United States
- R24 MH059724/MH/NIMH NIH HHS/United States
- R03 DA027513/DA/NIDA NIH HHS/United States
- P50 DA026306/DA/NIDA NIH HHS/United States
- U01 MH083500/MH/NIMH NIH HHS/United States
- U01 MH008021/MH/NIMH NIH HHS/United States
- U24 MH100928/MH/NIMH NIH HHS/United States
- P30 MH062512/MH/NIMH NIH HHS/United States
- U01 MH083545/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
