

Who should have surgery for spinal stenosis? Treatment effect predictors in SPORT
- PMID: 23018805
- PMCID: PMC3758127
- DOI: 10.1097/BRS.0b013e3182634b04
Who should have surgery for spinal stenosis? Treatment effect predictors in SPORT
Abstract
Study design: Combined prospective randomized controlled trial and observational cohort study of spinal stenosis (SpS) with an as-treated analysis.
Objective: To determine modifiers of the treatment effect (TE) of surgery (the difference between surgical and nonoperative outcomes) for SpS using subgroup analysis.
Summary of background data: The Spine Patient Outcomes Research Trial demonstrated a positive surgical TE for SpS at the group level. However, individual characteristics may affect TE. No previous studies have evaluated TE modifiers in SpS.
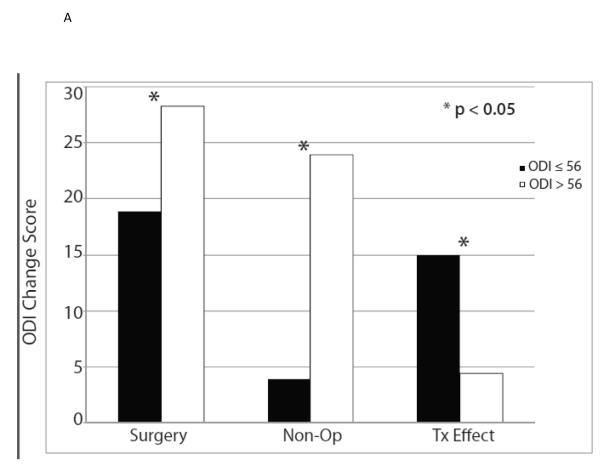
Methods: SpS patients were treated with either surgery (n = 419) or nonoperative care (n = 235) and were analyzed according to treatment received. Fifty-three baseline variables were used to define subgroups for calculating the time-weighted average TE for the Oswestry Disability Index (ODI) over 4 years (TE = ΔODIsurgery - ΔODInonoperative). Variables with significant subgroup × treatment interactions (P < 0.05) were simultaneously entered into a multivariate model to select independent TE predictors.
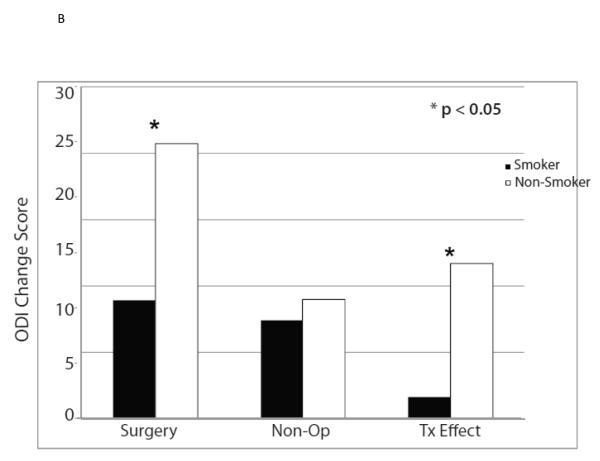
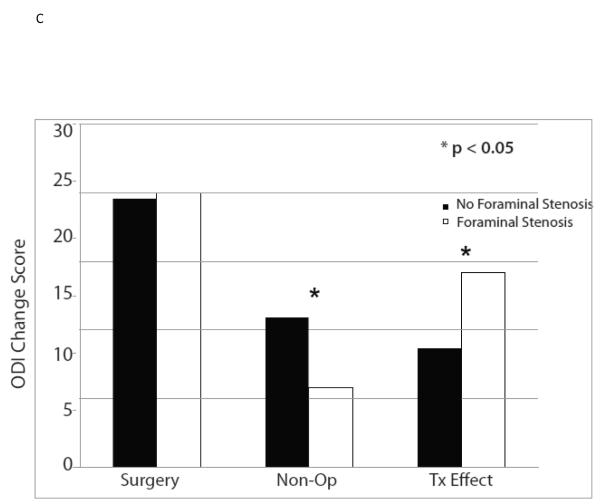
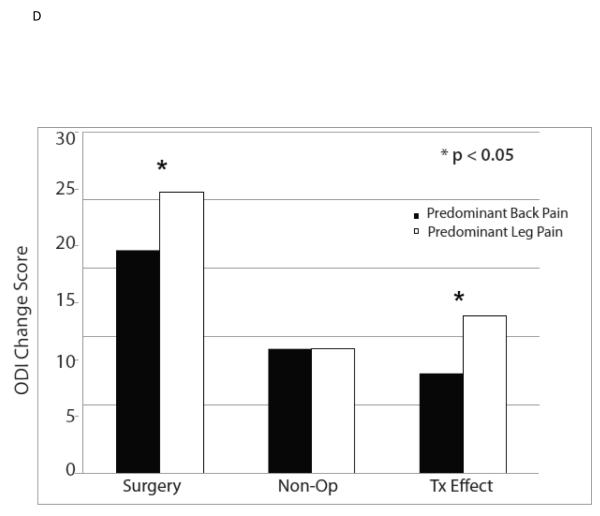
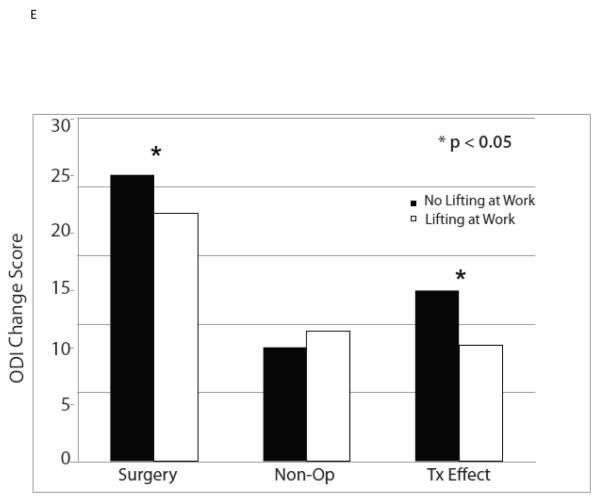
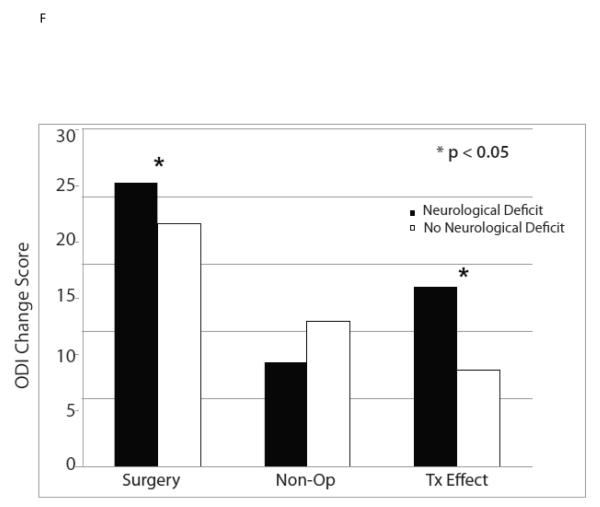
Results: Other than smokers, all analyzed subgroups including at least 50 patients improved significantly more with surgery than with nonoperative treatment (P < 0.05). Multivariate analysis demonstrated: baseline ODI ≤ 56 (TE -15.0 vs. -4.4, ODI > 56, P < 0.001), not smoking (TE -11.7 vs. -1.6 smokers, P < 0.001), neuroforaminal stenosis (TE -14.2 vs. -8.7 no neuroforaminal stenosis, P = 0.002), predominant leg pain (TE -11.5 vs. -7.3 predominant back pain, P = 0.035), not lifting at work (TE -12.5 vs. -0.5 lifting at work, P = 0.017), and the presence of a neurological deficit (TE -13.3 vs. -7.2 no neurological deficit, P < 0.001) were associated with greater TE.
Conclusion: With the exception of smokers, patients who met strict inclusion criteria improved more with surgery than with nonoperative treatment, regardless of other specific characteristics. However, TE varied significantly across certain subgroups, and these data can be used to individualize shared decision making discussions about likely outcomes. Smoking cessation should be considered before surgery for SpS.
Figures
References
-
- Atlas SJ, Deyo RA, Keller RB, et al. The Maine Lumbar Spine Study, Part III. 1-year outcomes of surgical and nonsurgical management of lumbar spinal stenosis. Spine. 1996;21:1787–94. discussion 94-5. - PubMed
-
- Atlas SJ, Keller RB, Robson D, Deyo RA, Singer DE. Surgical and nonsurgical management of lumbar spinal stenosis: four-year outcomes from the maine lumbar spine study. Spine. 2000;25:556–62. - PubMed
-
- Malmivaara A, Slatis P, Heliovaara M, et al. Surgical or nonoperative treatment for lumbar spinal stenosis? A randomized controlled trial. Spine. 2007;32:1–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
