

Plasma N-terminal pro-B-type natriuretic peptide is predictive of perioperative cardiac events in patients undergoing vascular surgery
- PMID: 23019395
- PMCID: PMC3443723
- DOI: 10.3904/kjim.2012.27.3.301
Plasma N-terminal pro-B-type natriuretic peptide is predictive of perioperative cardiac events in patients undergoing vascular surgery
Abstract
Background/aims: Identification of patients at high risk for perioperative cardiac events (POCE) is clinically important. This study aimed to determine whether preoperative measurement of plasma N-terminal pro-B-type natriuretic peptide (NT-proBNP) could predict POCE, and compared its predictive value with that of conventional cardiac risk factors and stress thallium scans in patients undergoing vascular surgery.
Methods: Patients scheduled for non-cardiac vascular surgery were prospectively enrolled. Clinical risk factors were identified, and NT-proBNP levels and stress thallium scans were obtained. POCE was the composite of acute myocardial infarction, congestive heart failure including acute pulmonary edema, and primary cardiac death within 5 days after surgery. A modified Revised Cardiac Risk Index (RCRI) was proposed and compared with NT-proBNP; a positive result for ischemia and a significant perfusion defect (≥ 3 walls, moderate to severely decreased, reversible perfusion defect) on the thallium scan were added to the RCRI.
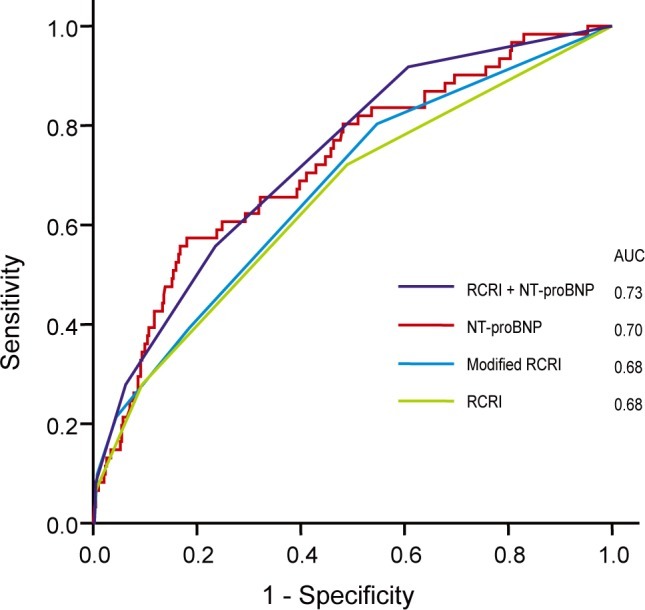
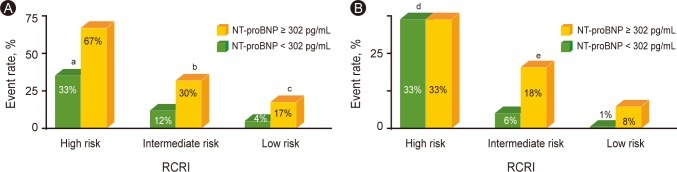
Results: A total of 365 patients (91% males) with a mean age of 67 years had a median NT-proBNP level of 105.1 pg/mL (range of quartile, 50.9 to 301.9). POCE occurred in 49 (13.4%) patients. After adjustment for confounders, an NT-proBNP level of > 302 pg/mL (odds ratio [OR], 5.7; 95% confidence interval [CI], 3.1 to 10.3; p < 0.001) and a high risk by the modified RCRI (OR, 3.9; 95% CI, 1.6 to 9.3; p = 0.002) were independent predictors for POCE. Comparison of the area under the curves for predicting POCE showed no statistical differences between NT-proBNP and RCRI.
Conclusions: Preoperative measurement of NT-proBNP provides information useful for prediction of POCE as a single parameter in high-risk patients undergoing noncardiac vascular surgery.
Keywords: Postoperative complications; Pro-B-type natriuretic peptide; Vascular surgical procedures.
Conflict of interest statement
No potential conflict of interest relevant to this article is reported.
Figures
References
-
- Landesberg G, Shatz V, Akopnik I, et al. Association of cardiac troponin, CK-MB, and postoperative myocardial ischemia with long-term survival after major vascular surgery. J Am Coll Cardiol. 2003;42:1547–1554. - PubMed
-
- Raby KE, Barry J, Creager MA, Cook EF, Weisberg MC, Goldman L. Detection and significance of intraoperative and postoperative myocardial ischemia in peripheral vascular surgery. JAMA. 1992;268:222–227. - PubMed
-
- Pasternack PF, Grossi EA, Baumann FG, et al. Silent myocardial ischemia monitoring predicts late as well as perioperative cardiac events in patients undergoing vascular surgery. J Vasc Surg. 1992;16:171–179. - PubMed
-
- Sprung J, Abdelmalak B, Gottlieb A, et al. Analysis of risk factors for myocardial infarction and cardiac mortality after major vascular surgery. Anesthesiology. 2000;93:129–140. - PubMed
-
- Bartels C, Bechtel JF, Hossmann V, Horsch S. Cardiac risk stratification for high-risk vascular surgery. Circulation. 1997;95:2473–2475. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials