

A case of severe coronary spasm associated with 5-fluorouracil chemotherapy
- PMID: 23019400
- PMCID: PMC3443728
- DOI: 10.3904/kjim.2012.27.3.342
A case of severe coronary spasm associated with 5-fluorouracil chemotherapy
Abstract
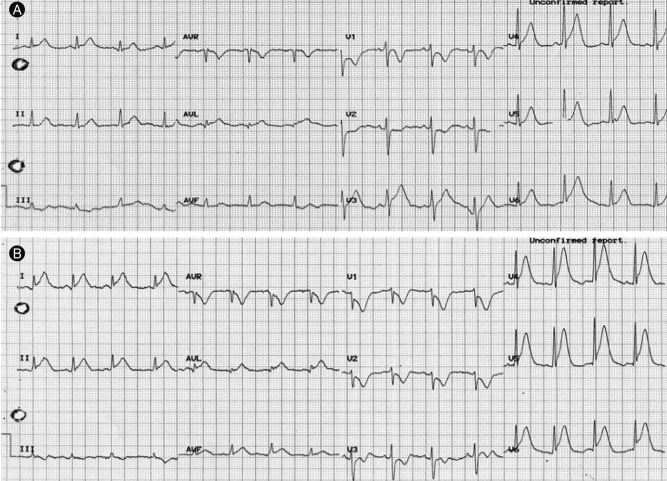
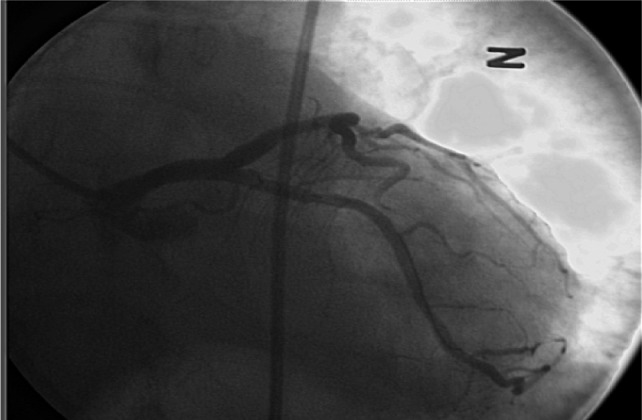
Cardiotoxicity associated with 5-fluorouracil (FU) is an uncommon, but potentially lethal, condition. The case of an 83-year-old man with colon cancer who developed chest pain during 5-FU infusion is presented. The electrocardiogram (ECG) showed pronounced ST elevation in the lateral leads, and the chest pain was resolved after infusion of nitroglycerin. A coronary angiogram (CAG) revealed that the patient had significant atherosclerosis in the proximal left circumflex artery. Coronary artery spasm with fixed stenosis was considered, and a drug-eluting stent was implanted. After 8 hours, the patient complained of recurring chest pain, paralleled by ST elevation on the ECG. The chest pain subsided after administration of intravenous nitroglycerin followed by sublingual nifedipine. Repeated CAG showed patency of the previous stent. This case supports the vasospastic hypothesis of 5-FU cardiac toxicity, indicating that a calcium channel blocker may be effective in the prevention or treatment of 5-FU cardiotoxicity.
Keywords: Angina pectoris; Calcium channel blockers; Coronary vasospasm; Fluorouracil.
Conflict of interest statement
No potential conflict of interest relevant to this article is reported.
Figures


References
-
- Jensen SA, Sorensen JB. Risk factors and prevention of cardiotoxicity induced by 5-fluorouracil or capecitabine. Cancer Chemother Pharmacol. 2006;58:487–493. - PubMed
-
- Wacker A, Lersch C, Scherpinski U, Reindl L, Seyfarth M. High incidence of angina pectoris in patients treated with 5-fluorouracil: a planned surveillance study with 102 patients. Oncology. 2003;65:108–112. - PubMed
-
- Robben NC, Pippas AW, Moore JO. The syndrome of 5-fluorouracil cardiotoxicity: an elusive cardiopathy. Cancer. 1993;71:493–509. - PubMed
-
- Kuzel T, Esparaz B, Green D, Kies M. Thrombogenicity of intravenous 5-f luorouracil alone or in combination with cisplatin. Cancer. 1990;65:885–889. - PubMed
-
- Gradishar WJ, Vokes EE. 5-Fluorouracil cardiotoxicity: a critical review. Ann Oncol. 1990;1:409–414. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources