

Quantitative analysis of the human airway microbial ecology reveals a pervasive signature for cystic fibrosis
- PMID: 23019655
- PMCID: PMC3898170
- DOI: 10.1126/scitranslmed.3004458
Quantitative analysis of the human airway microbial ecology reveals a pervasive signature for cystic fibrosis
Abstract
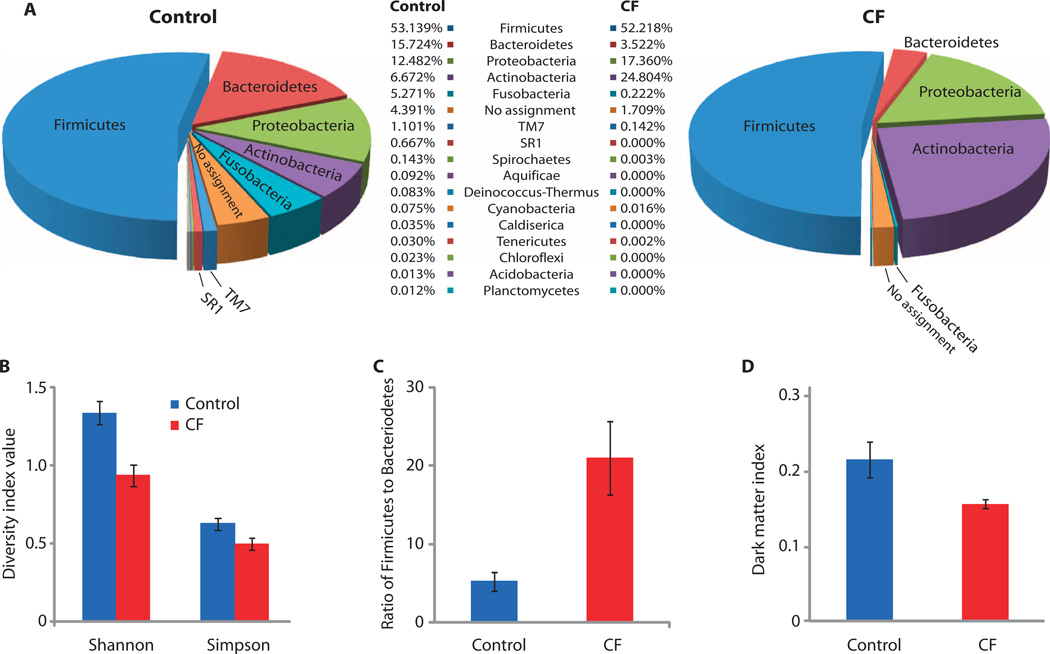
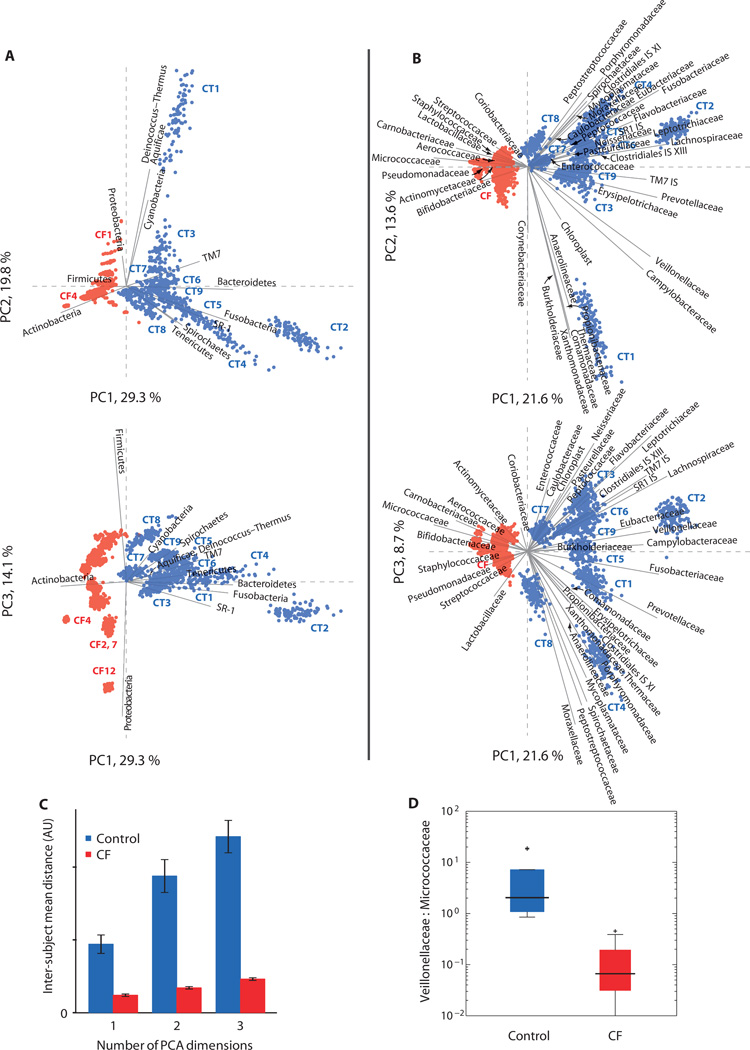
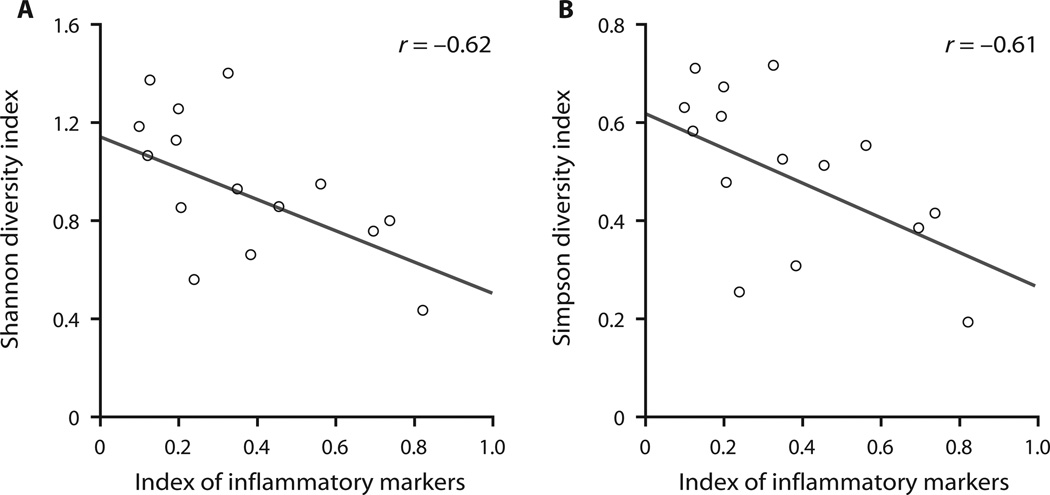
Cystic fibrosis (CF) is an autosomal recessive disease caused by mutations in the gene encoding the CF transmembrane conductance regulator. Disruption of electrolyte homeostasis at mucosal surfaces leads to severe lung, pancreatic, intestinal, hepatic, and reproductive abnormalities. Loss of lung function as a result of chronic lung disease is the primary cause of death from CF. Using high-throughput sequencing to survey microbes in the sputum of 16 CF patients and 9 control individuals, we identified diverse microbial communities in the healthy samples, contravening conventional wisdom that healthy airways are not significantly colonized. Comparing these communities with those from the CF patients revealed significant differences in microbial ecology, including differential representation of uncultivated phylotypes. Despite patient-specific differences, our analysis revealed a focal microbial profile characteristic of CF. The profile differentiated case and control groups even when classically recognized CF pathogens were excluded. As a control, lung explant tissues were also processed from a group of patients with pulmonary disease. The findings in lung tissue corroborated the presence of taxa identified in the sputum samples. Comparing the sequencing results with clinical data indicated that diminished microbial diversity is associated with severity of pulmonary inflammation within our adult CF cohort.
Figures
References
-
- Gibson RL, Burns JL, Ramsey BW. Pathophysiology and management of pulmonary infections in cystic fibrosis. Am. J. Respir. Crit. Care Med. 2003;168:918–951. - PubMed
-
- Harrison F. Microbial ecology of the cystic fibrosis lung. Microbiology. 2007;153:917–923. - PubMed
-
- di Sant’agnese PA, Davis PB. Cystic fibrosis in adults, 75 cases and a review of 232 cases in the literature. Am. J. Med. 1979;66:121–132. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
